Trends
Sci.
2026;
23(10):
13458
Evaluation of Anti-Ulcerogenic Effect of Castanopsis costata Extract Against Experimental Gastric Ulcer in Rats
Maulana Yusuf Alkandahri1,*, Asman Sadino2, Wilda Fhitriany Usman3, Zulpakor Oktoba4, Aprilya Sri Rachmayanti5, Rastria Meilanda6, Ermi Abriyani7, Dani Sujana8,
Andi Nurzakiah Amal1 and Sigit Roma Rezki Harahap9
1Department of Pharmacology and Clinical Pharmacy, Faculty of Pharmacy,
Universitas Buana Perjuangan Karawang, Karawang, Indonesia
2Department of Pharmacy, Faculty of Mathematics and Natural Sciences, Universitas Garut, Garut, Indonesia
3Pharmacist Professional Education Study Program, Faculty of Pharmacy, Universitas Islam Sultan Agung,
Semarang, Indonesia
4Department of Pharmacy, Faculty of Medicine, Universitas Lampung, Bandar Lampung, Indonesia
5Pharmacist Professional Education Study Program, Institut Kesehatan Mitra Bunda, Batam, Indonesia
6Department of Pharmacy, Institut Kesehatan Mitra Bunda, Batam, Indonesia
7Department of Pharmaceutical Chemistry, Faculty of Pharmacy, Universitas Buana Perjuangan Karawang, Karawang, Indonesia
8Diploma Program of Pharmacy, Karsa Husada Garut College of Health Sciences, Garut, Indonesia
9Faculty of Pharmacy, Universitas Buana Perjuangan Karawang, Karawang, Indonesia
(*Corresponding author’s e-mail: [email protected])
Received: 26 January 2026, Revised: 4 March 2026, Accepted: 11 March 2026, Published: 30 April 2026
Abstract
Gastrointestinal diseases, such as gastric ulcer (GU), are caused by damage to the GM, alcohol consumption, NSAIDs (specifically ketorolac), and Helicobacter pylori. Currently, several plants are effective in treating GU, including Castanopsis costata. Until now, there has been no report regarding the antiulcerogenic effects of ethanolic extract of C. costata (EECc) reported. Therefore, this research aimed to test antiulcerogenic potential of EECc in 3 rat models of GU induced by ethanol (EtOH) 1 mL orally, ketorolac (30 mg/kg orally), and H. pylori (1.0×109 CFU intragastrically). Each treatment group in the experimental model was given EECc 50, 100, and 200 mg/kg orally. In this context, GpH and GV, FA and TA, as well as UI, were measured to assess gastric function. Measurements of inflammatory cytokines levels, as well as histopathological examination of tissue, were carried out to determine the effects of organ damage. Anti-H. pylori activity was tested in vitro and in vivo to assess the inhibition of H. pylori growth. The results showed that EECc improved gastric function, reduced the levels of TNF-α, IL-1β, and IL-6, increased PGE2, inhibited the growth of H. pylori in vitro and in vivo, and improved tissue architecture by reducing the severity of GM injury, leukocyte infiltration, and bleeding. Moreover, EECc had antiulcerogenic effects in EtOH-, ketorolac-, and H. pylori-induced GU rat models.
Keywords: Castanopsis costata, Antiulcerogenic, Ethanol, Ketorolac, Helicobacter pylori
Introduction
Gastric ulcer (GU) is a wound or lesion sustained due to a tear in the lining of the gastric mucosa (GM) that extends to the entire muscularis mucosa. This wound is characterized by various stages, including necrosis, increased oxidative stress, leukocyte infiltration, decreased blood flow, and inflammation [1]. Furthermore, GU occurs due to an imbalance between mucosal defense factors, including mucus secretion,
prostaglandin E2 (PGE2) synthesis, endogenous antioxidants, bicarbonate efflux, nitric oxide (NO), and sulfhydryl compounds (SH) as well as detrimental aggressive factors, namely pepsin, hydrochloric acid, smoking, stress, excessive alcohol consumption, use of NSAIDs, and H. pylori infection [2,3]. The most common causes of GM damage include heavy alcohol consumption, use of NSAIDs (specifically ketorolac), and H. pylori infection [4,5]. Most people with GU experience common symptoms such as abdominal discomfort, nausea, epigastric pain, vomiting, and a gnawing or burning sensation after eating. The complications are bleeding, perforation, and pyloric obstruction [6]. Globally, the number of GU cases has reached 2,854,370 with 230,217 deaths [7]. The disease occurs with a high recurrence rate and requires a long treatment period [8]. Several conventional medications are used to protect and repair GM damage in sufferers, such as histamine type-2 receptor antagonists (ranitidine), M1 receptor antagonists (pirenzepine), PPIs (omeprazole), antimicrobial agents (clarithromycin), and prostaglandin analogs (misoprostol) [9,10]. The medications have several side effects, including gynecomastia, impotence, osteoporosis, anaphylactic reactions, acute interstitial nephritis, and iron, magnesium, and vitamin B12 deficiencies [10,11]. Therefore, alternative treatments are needed to develop more effective agents, prevent recurrence, and minimize side effects [12].
Medicinal plants have long been used to treat digestive system diseases in multiple countries, including Indonesia [13,14]. This is because medicinal plants have various pharmacological activities and chemical compounds, milder side effects in long-term use compared to synthetic drugs, widespread availability, and low toxicity [15,16]. Indonesia is the country possessing the 2nd-highest biodiversity, with thirty thousand plant species successfully documented. A total of 6,000 medicinal plants are considered, including Castanopsis costata [17-19]. Empirically, C. costata leaves are often used to treat various digestive disorders, analgesic, and inflammation [20]. Several previous research reported that ethanolic extract of C. costata (EECc) had multiple biological activities, including antimalarial [21], antidiabetic [22], antioxidant [23], antihyperlipidemic [24], antidiarrheal [19], analgesic [25], anti-inflammatory [25], hepatoprotective [26], and nephroprotective [26]. Medicinal plants with antioxidant and anti-inflammatory activities possess anti-gastric ulcer effects [27,28]. Antioxidant compounds are reported to counteract and clean free radicals, such as ROS that play a role in the induction of ulcer, as well as stimulate the formation of prostaglandins to increase healing and protect the gastric mucosa from injury [29,30]. Anti-inflammatory compounds have been reported to reduce inflammatory cytokines formed in GU to increase healing and prevent recurrence [31]. Based on previous research, EECc was reported to have antioxidant and anti-inflammatory activities. Furthermore, EECc is also reported to have high phenolic and flavonoid compounds, where these compounds can act as antiulcerogenic by neutralizing ROS, increasing endogenous antioxidant enzymes, reducing lipid peroxidation levels, stimulating mucus production, strengthening the gastric barrier, increasing prostaglandin production (PGE2), inhibiting acid secretion, decreasing the release of inflammatory cytokines (such as TNF-α, IL-1β, and IL-6) and inhibiting the growth of H. pylori [32-34]. The pharmacological activities and phytochemical compounds of EECc can strengthen the hypothesis that EECc also has the potential to possess antiulcerogenic activity. On the other hand, until now, there has been no report regarding the antiulcerogenic effects of EECc reported, so this could provide a novelty in the discovery of antiulcer agents derived from medicinal plants. Therefore, this research aims to examine antiulcerogenic potential of EECc in ethanol (EtOH)-induced, ketorolac-induced, and H. pylori-induced GU.
Materials and methods
Materials and bacterial
Omeprazole (PT. Novell Pharmaceutical Laboratories, Indonesia), ketorolac (PT. Kalbe Farma, Indonesia), clarithromycin (PT. Sanbe Farma, Indonesia), amoxicillin (PT. Kalbe Farma, Indonesia), 0.9% sodium chloride (PT. B. Braun Pharmaceutical, Indonesia), ethyl ether (PT. Bratachem, Indonesia), Topfer reagent (HiMedia Laboratories, India), paraffin, mueller-hinton broth, phosphate buffered saline, sodium hydroxide, 80% ethanol, 10% formalin solution, hematoxylin-eosin stains, 70% ethanol, fetal bovine serum (FBS), xylene, phenolphthalein, pulvis gummi arabicum (EMSURE® ACS Merck, Germany). TNF-α ELISA kits (MBS175787), IL-1β ELISA kits (MBS2023030), IL-6 ELISA kits (MBS2020158), PGE2 ELISA kits (MBS1603501) (MyBioSource, Inc. San Diego, USA). Bacterial cultures were purchased from BEI Resources (NIAID, USA): Helicobacter pylori CPY6081 (cat. no. NR-43639).
Plant materials, determination, and extract preparation
Approximately 15 kg of fresh leaves were collected from Pancur Batu Region in Medan, Indonesia. The plants were identified at Herbarium Jatinangor, Universitas Padjadjaran (voucher number: 488/LBM/IT/I/2025; collection number: 607). The fresh leaves were collected, cleaned with water, cut into small pieces, and dried. After the leaves were ground into a powder, 3 kg were macerated for 3×24 h in 70% EtOH. A rotary evaporator was used to collect and concentrate the liquid extract at 55 °C [35].
Randomization procedure, blinding, and experimental replicates
For randomization, an identification number was first assigned to each rat and then randomization was performed, which generated random numbers and allocated rats to study groups. Randomization was performed using online software (https://www.graphpad.com/quickcalcs/randomize1/). Meanwhile, in blinding during the experiment, alphanumeric codes were used to identify vials and syringes and each rat was given a number. Then, each sample code was placed in a sealed envelope and revealed at the end of the experiment. Sample size determination was based on Federer calculation formula, which is (t - 1) (n - 1) ≥ 15; where “t” is the number of the groups and “n” is the experimental animal per group. (6 - 1) (n - 1) ≥ 15 → n ≥ 4, for the testing of EtOH-, ketorolac-, and H. pylori-induced GU in rats. According to this calculation, the minimum sample size was 4 experimental animals in each treatment and control group.
Experimental animals
The male Wistar rats (a total of 120), ages 10 - 12 weeks and 200 - 250 g, were used in this research. Rats were kept in the Pharmacology and Toxicology Laboratory at Universitas Buana Perjuangan Karawang after being acquired from the CV. Mitra Putra Animal, West Java, Indonesia. Every experimental animal had ad libitum access to standard pellets and water, and they were all kept in polypropylene cages with softwood shavings under standard housing circumstances (12-hour light/dark cycle, 25 ± 3 °C room temperature, and 55 ± 5% humidity). The Research Ethics Commission of Universitas Padjadjaran, Indonesia, accepted this protocol under the number: 499/UN6.KEP/EC/2024 (May 2, 2024), in compliance with ARRIVE guidelines.
Protocol for antiulcerogenic activity
EtOH-induced GU in rats
In this research, antiulcerogenic activity was tested using an EtOH-induced GU model. The experimental animals were randomly divided into 6 groups (n = 5). Group 1 - 3 acted as normal (healthy), NC (ulcerated with EtOH and not treated), and positive (ulcerated with EtOH and treated with OMP 20) controls, respectively. Meanwhile, Groups 4 - 6 acted as test groups (ulcerated with EtOH and treated with EECc 50, EECc 100, and EECc 200). OMP and EECc were administered orally for fourteen days before GU induction with EtOH. On the 15th day, rats in all treatment groups (except the normal control) received 80% EtOH (1 mL/rat) orally to induce GU. After an hour, the animals were anesthetized with cotton balls saturated with 1.9% ethyl ether in a small chamber for 2 to 5 min and euthanized by cervical dislocation. The stomachs were removed to examine the test parameters of each experimental group [36,37].
Ketorolac-induced GU in rats
The further test of antiulcerogenic activity was conducted using a ketorolac-induced GU model. The experimental animals were divided into 6 groups (n = 5). Groups 1 - 3 served as the normal (healthy), NC (ulcerated with ketorolac and not treated), and positive (rats ulcerated with ketorolac and treated with OMP 20) controls, respectively. Meanwhile, Groups 4 - 6 acted as test groups (ulcerated with ketorolac and treated with EECc 50, EECc 100, and EECc 200). OMP and EECc were administered orally one hour before GU induction with ketorolac. Rats in all treatment groups (except in the normal control) received 30 mg/kg ketorolac to induce GU. After eighteen hours of ulcer induction, all rats were anesthetized with cotton balls saturated with 1.9% ethyl ether in a small chamber for 2 to 5 min and euthanized by cervical dislocation. Subsequently, the stomachs were removed to examine the test parameters of each experimental group [38].
Bacterial strain
Before testing antibacterial activity of EECc against H. pylori, an inoculum of the bacterial strain (Helicobacter pylori CPY6081) was prepared from an overnight broth culture. The suspension was adjusted to a McFarland standard turbidity of 0.5 (equivalent to 1.0×108 CFU/mL, as per the consensus standard of the CLSI) [39].
Anti-H. pylori activity
The stock solutions of EECc and clarithromycin were filtered through a pyrogenic filter to sterilize the solutions before experimenting. Furthermore, serial dilution was carried out to various concentrations of 200 - 12.5 µg/mL and 0.001 - 10 µg/mL for EECc and clarithromycin, respectively. A 96-well plate was prepared, and 100 µL of MHB, 20 µL of inoculum, EECc, and clarithromycin were poured into each well. Microorganism growth was determined by the presence of turbidity, and clear wells indicated no bacterial growth. MIC of the test sample was the lowest in the medium that completely inhibited visible bacterial growth. In addition, 100 µL samples were taken from tubes without visible bacterial growth during MIC test and infused into MHB in sterile wells to determine MBC. The plates were incubated at 37 °C for 24 h in a microaerophilic environment (10% Carbon dioxide, 5% Oxygen). MBC was defined as the lowest concentration without producing bacterial growth in the experiment [40].
H. pylori-induced GU in rats
Before performing an antiulcerogenic test, H. pylori was first cultured in brain-heart infusion broth with 10% FBS for an entire night at 37 °C in a microaerophilic environment until it reached a density of 2.0×109 CFU/mL. Subsequently, this bacterium was inoculated, suspended in 0.5 mL of broth (containing 1.0×109 CFU H. pylori), into the test rats intragastrically (i.g.) 3 times with an interval of 3 days for 4 weeks. To determine the test rats positively infected with H. pylori, fecal antigen analysis was carried out with the SD Bioline H. pylori Ag kit. The test rats were divided into 6 groups (n = 10). Groups 1 - 3 acted as normal (healthy), NC (infected with H. pylori and not treated), and positive [infected with H. pylori and treated with triple therapy (TT) (CLA 25, AMOX 50, and OMP 20)] controls, respectively. Meanwhile, Groups 4 - 6 acted as test groups (rats infected with H. pylori and treated with EECc 50, EECc 100, and EECc 200 daily orally for 4 weeks). On the final day, all rats were anesthetized with cotton balls saturated with 1.9% ethyl ether in a small chamber for 2 to 5 min and euthanized by cervical dislocation. The stomachs were removed to examine the test parameters of each experimental group. To detect H. pylori colonization, half of the glandular mucosa was scraped. According to the protocol described by Santiago et al., H. pylori colonization was confirmed with a rapid urease test [41].
Determination of antiulcerogenic activity
Evaluation of stomachs
In all experimental models, rats’ stomachs were opened along the larger curvature and cleaned with a NaCl (0.9%) solution to remove blood clots and gastric contents. In order to evaluate ulcer formation, each stomach was inspected using a 10× magnification lens. The index could be measured using the score described by Ahmed et al. [10].
Ulcer severity score:
Normal = 0; bleeding spots = 0.5; mild inflammation = 1; moderate inflammation = 2; heavy bleeding = 3; perforation = 4.
Gastric pH (GpH) and gastric volume (GV)
Gastric juice was taken from the stomachs of rats in each experimental model, transferred into a measuring tube, centrifuged for 10 min at 4,000 rpm, and the volume of the supernatant was measured. Furthermore, 1 mL of distilled water was added to dilute the fluid, and a pH meter was used to determine its pH [42].
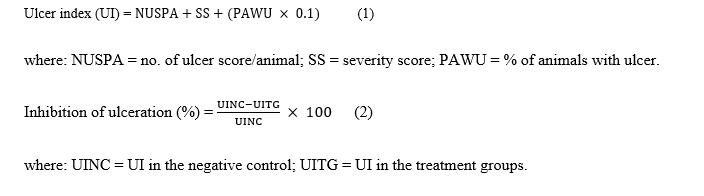
Free acidity (FA) and total acidity (TA)
The diluted gastric juice with 0.01 N NaOH was titrated using Topfer’s reagent and 1% phenolphthalein to determine the FA and TA levels of gastric juice in each experimental model. The volume of sodium hydroxide reflected the amount of FA and TA in the gastric juice and was expressed in mEq/L. In this context, acidity was calculated using the formula below:

Determination of inflammatory cytokines
Rat gastric tissue segments in each experimental model were taken, homogenized with ninefold ice-cold PBS, and centrifuged for 15 min at 6,000 rpm to determine inflammatory cytokine levels. The supernatant was collected, and the levels of TNF-α, IL-1β, IL-6, and PGE2 in gastric homogenates were determined using an ELISA kit (MyBioSource, Inc.), according to the manufacturer’s instructions. An automated microplate reader (ELx50; BioTek, Agilent Technologies, Inc.) was used to measure the optical density at 450 nm.
Histopathological observation of gastric tissue
Gastric tissue samples from each experimental model were washed and cleaned with 0.9% NaCl for 48 - 72 h in 10% formalin solution. Subsequently, the samples were processed through alcohol dehydration, followed by xylene cleaning and paraffin infiltration. Paraffin-embedded tissue blocks were cut with a thickness of 5 micrometers using a rotary microtome, then dried and fixed on glass slides. The slides were deparaffinized with xylene for 30 min and dehydrated with a hot plate for 5 min. The sections were stained with H&E. The slides were observed using Olympus BX-51 (a light microscope) equipped with a camera (Olympus Q Color-5) connected to a computer and a 100× objective lens. Histopathological alterations were assessed using a standardized nonlinear semiquantitative scoring method and a scale ranging from 0 to 4, as adapted from Eltahir, with minor modifications. Significant findings were scored: 0 = no change; 1 = <25% tissue damage; 2 = 26% - 50% tissue damage; 3 = 51% - 75% tissue damage; 4 = 76% - 100% tissue damage [43].
Statistical evaluation
All experiment data were presented as mean ± SEM. Using GraphPad Prism version 10, one-way ANOVA and Tukey’s post hoc test were used to analyze differences between the means of the measured parameters. p < 0.05 were deemed significant.
Results and discussion
Effect of EECc on gastric juice parameters in EtOH-induced GU rats
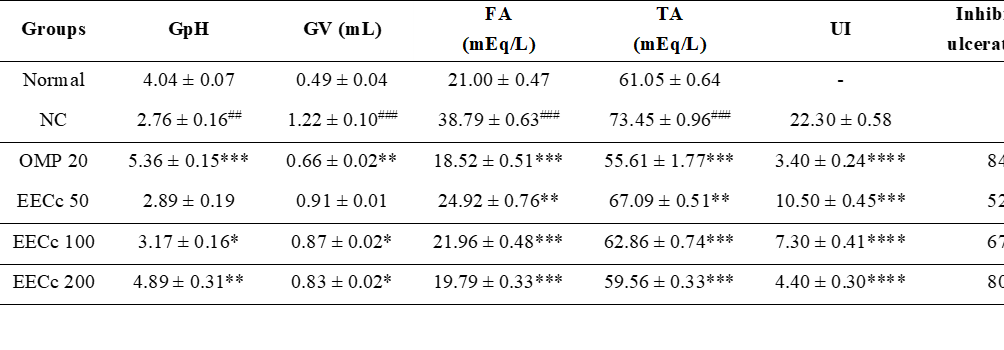
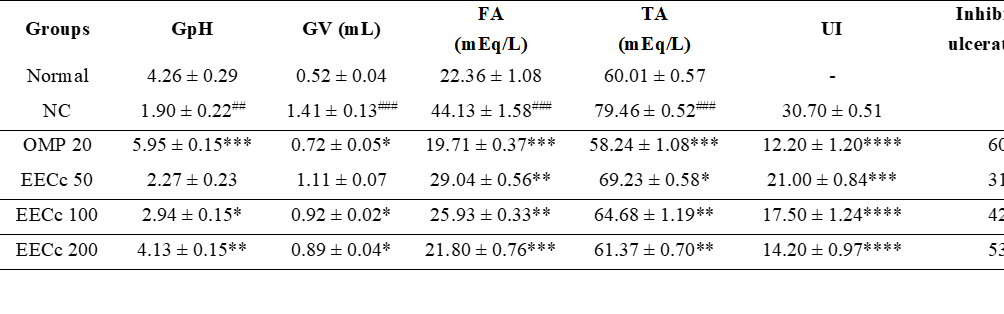
Based on the results, the administration of 80% EtOH at 1 mL/rat decreased GpH and significantly increased GV, FA, and TA (p < 0.01 - p < 0.001). Meanwhile, the administration of EECc 100 and EECc 200 caused a significant increase (p < 0.05 - p < 0.01) in GpH and decrease (p < 0.05 - p < 0.001) in GV, FA, and TA in EtOH-induced GU rats. Meanwhile, EECc 50 only caused a significant decrease in FA (p < 0.01) and TA (p < 0.01). The results confirmed that administering OMP had a better effect on changes in gastric juice parameters (p < 0.01 - p < 0.001) than EECc. The administration of EECc at all doses, as well as OMP, had a significantly lower UI (p < 0.001 - p < 0.0001) and an inhibition percentage of 52.64%, 67.34%, 80.14%, and 84.73%, respectively. Table 1 shows the effect of EECc administration on gastric juice parameters, UI, and % inhibition of ulceration in EtOH-induced GU rats.
Table 1 The effect of EECc on GpH, GV, FA, TA, UI, and % inhibition of ulceration in EtOH-induced GU rats.
All
experiment data were presented as mean ± SEM (n
= 5). *p
< 0.05, **p
< 0.01, ***p
< 0.001, ****p
< 0.0001 vs. the NC. ##p
<
0.01, ###p
< 0.001 vs. the normal group. NC, negative control.
Effect of EECc on inflammatory cytokines levels in EtOH-induced GU rats
Based on the results, administration of 80% EtOH at 1 mL/rat caused an increase in TNF-α, IL-1β, and IL-6 and a significant decrease in PGE2 levels (p < 0.0001). Meanwhile, EECc at all doses decreased in TNF-α (p < 0.05 - p < 0.001), IL-1β (p < 0.01 - p < 0.0001), and IL-6 (p < 0.01 - p < 0.0001), as well as increased PGE2 levels (p < 0.05 - p < 0.01) in EtOH-induced GU rats. OMP decreased TNF-α, IL-1β, and IL-6, as well as increased PGE2 levels, which were not significantly different when compared to NC (p > 0.05). The results showed that EECc was more effective in influencing changes in the inflammatory cytokine levels of EtOH-induced GU rats than OMP. Figure 1 shows the effect of EECc on inflammatory cytokine levels in EtOH-induced GU rats.
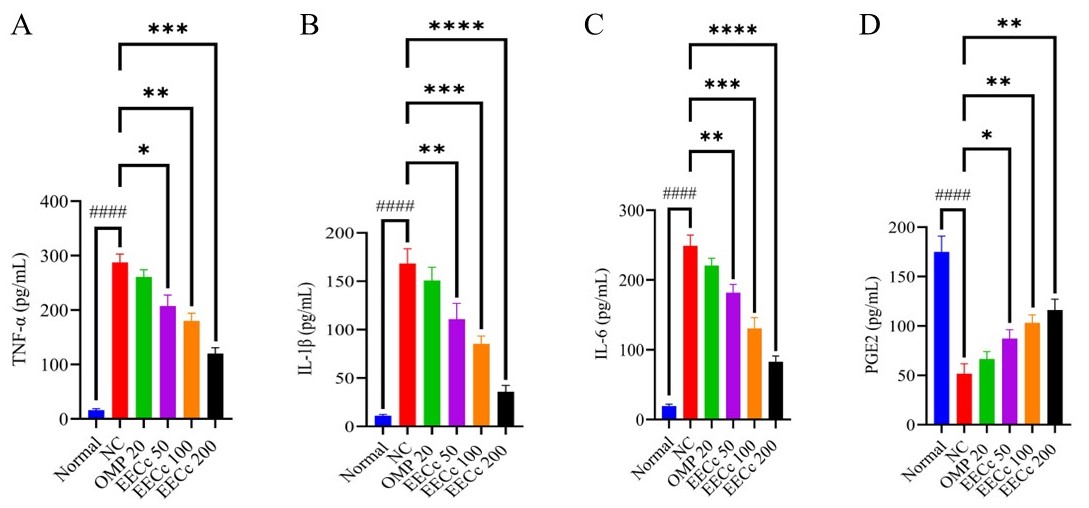
Figure 1 Effect of EECc on inflammatory cytokines levels in EtOH-induced GU rats. All experiment data were presented as mean ± SEM (n = 5). *p < 0.05, **p < 0.01, ***p < 0.001, ****p < 0.0001 vs. the NC. ####p < 0.0001 vs. the normal group. NC, negative control.
Effect of EECc on histopathological observation of gastric tissue in EtOH-induced GU rats
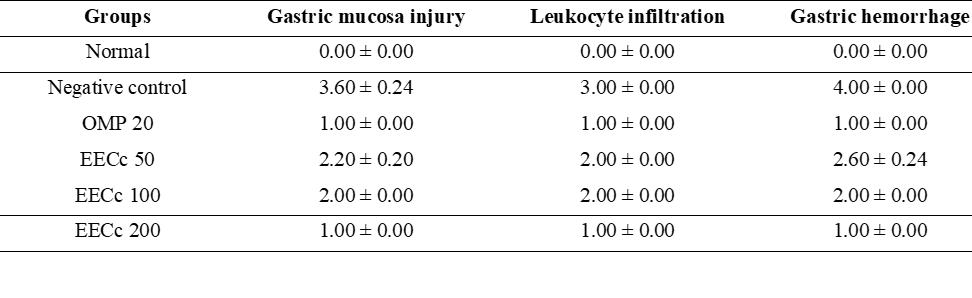
Based on histopathological observation of the gastric tissue, there was an intact mucosal layer structure with a regular epithelial arrangement and no evidence of desquamation or damage to the glands (Figure 2(A)). In the NC group, there was injury to the GM, as seen from epithelial desquamation and damage to the glandular layer. Additionally, several leukocyte infiltration was reported in the lamina propria, indicating an active inflammatory response. An accumulation of erythrocytes outside the blood vessels also reported GM bleeding (Figure 2(B)). The treatment group given OMP showed injury to the GM in the form of mild desquamation and a reduction in glands, as well as leukocyte infiltration in smaller numbers (Figure 2(C)). The administration of EECc at all doses showed mild erosion in the GM and the structure was relatively intact. However, necrosis was visible, leukocyte infiltration was mild in a small area, and bleeding was slight and not massive (Figures 2(D) - 2(F)). The histopathological scores of the gastric tissue of rats with EtOH-induced GU are displayed in Table 2.
Table 2 Effect of EECc on histopathological scoring of gastric tissue in EtOH-induced GU rats.
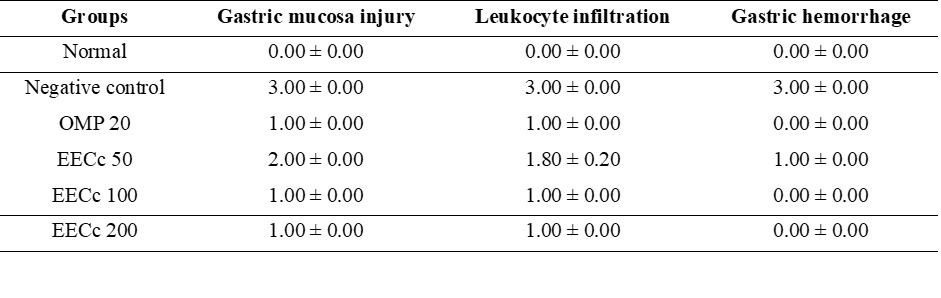
The
data are presented as mean ±
SEM (n
= 5).
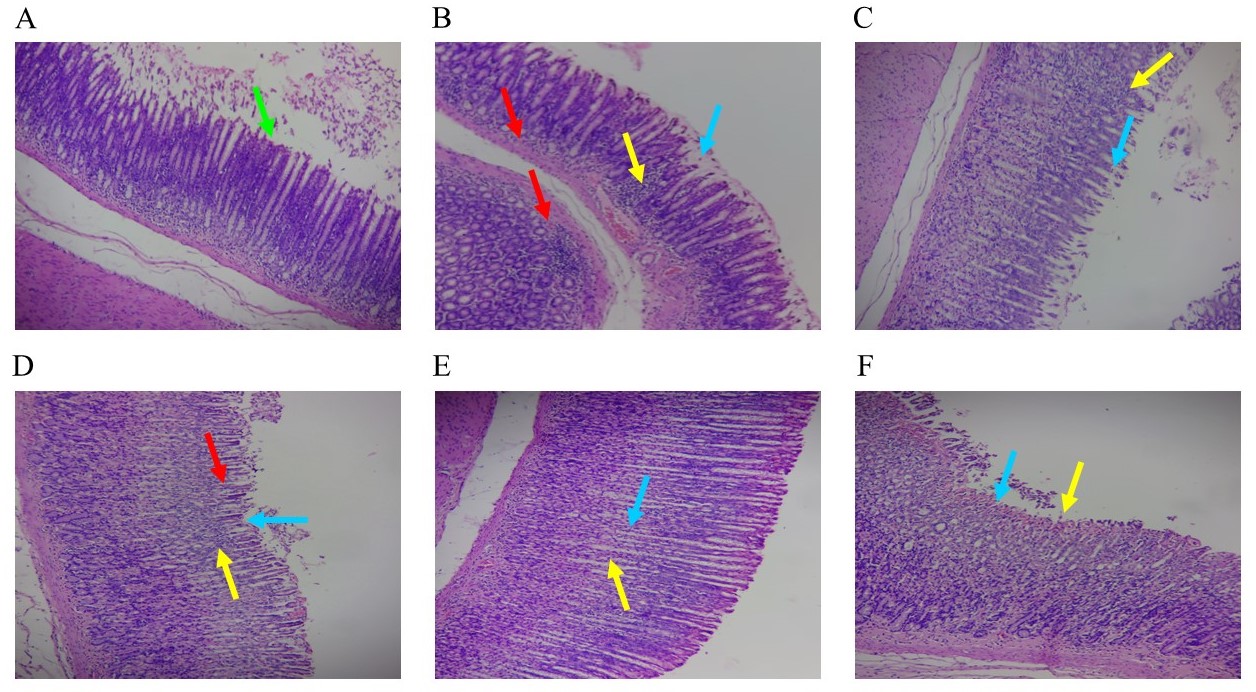
Figure 2 The effect of EECc on histopathological appearance of gastric tissue in EtOH-induced GU rats. (A) Normal. (B) NC. (C) OMP 20. (D) EECc 50. (E) EECc 100. (F) EECc 200. Light green arrow (gastric mucosa); Light blue arrows (gastric mucosa injury); Yellow arrows (leucocytes infiltration); Red arrows (gastric hemorrhage). Magnification, ×100 and stained with H&E.
Effect of EECc on gastric juice parameters in ketorolac-induced GU rats
The administration of ketorolac at 30 mg/kg in rats caused a decrease in GpH and increase in GV, FA and TA (p < 0.01 - p < 0.001). EECc 100 and EECc 200 increased (p < 0.05 - p < 0.01) GpH and decreased (p < 0.05 - p < 0.001) GV, FA, and TA in ketorolac-induced GU rats. Meanwhile, the EECc 50 only decreased FA (p < 0.01) and TA (p < 0.05). The administration of OMP was reported to have a better effect on changes in gastric juice parameters (p < 0.05 - p < 0.001) than EECc. The results showed that EECc at all doses, as well as OMP, had a significantly lower UI (p < 0.001 - p < 0.0001) and had ulcer inhibition percentages of 31.63%, 42.87%, 53.53%, and 60.16%, respectively. Table 3 shows the effect of EECc administration on gastric juice parameters, UI, and % inhibition of ulceration in ketorolac-induced GU rats.
Table 3 The effect of EECc on GpH, GV, FA, TA, UI, and % inhibition of ulceration in ketorolac-induced GU rats.
All
experiment data were presented as mean ± SEM (n
= 5). *p
< 0.05, **p
< 0.01, ***p
< 0.001, ****p
< 0.0001 vs. the NC. ##p
< 0.01, ###p
< 0.001 vs. the normal group. NC, negative control.
Effect of EECc on inflammatory cytokines levels in ketorolac-induced GU rats
The administration of ketorolac at 30 mg/kg increased TNF-α, IL-1β, and IL-6, and decreased PGE2 levels (p < 0.0001). EECc at all doses was reported to decrease TNF-α (p < 0.05 - p < 0.001), IL-1β (p < 0.01 - p < 0.001), and IL-6 (p < 0.05 - p < 0.001), as well as increase PGE2 levels (p < 0.05 - p < 0.01) in ketorolac-induced GU rats. Meanwhile, OMP decreased TNF-α, IL-1β, and IL-6, as well as increased PGE2 levels, which were not significantly different when compared to NC (p > 0.05). The results showed that EECc had a better effect in influencing changes in the inflammatory cytokine levels of ketorolac-induced GU rats than OMP. Figure 3 shows the effect of EECc on inflammatory cytokine levels in ketorolac-induced GU rats.
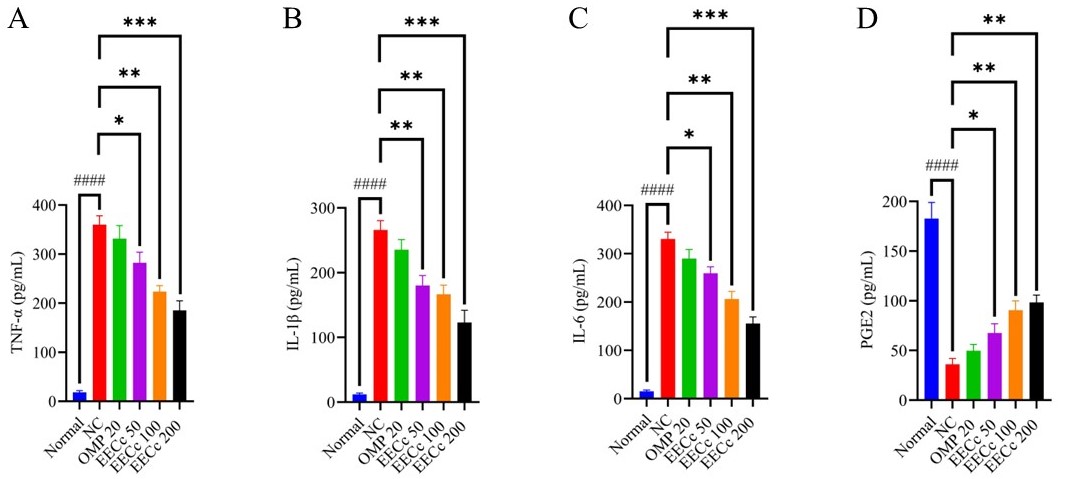
Figure 3 Effect of EECc on inflammatory cytokines levels in ketorolac-induced GU rats. All experiment data were presented as mean ± SEM (n = 5). *p < 0.05, **p < 0.01, ***p < 0.001 vs. the NC group. ####p < 0.0001 vs. the normal group. NC, negative control.
Effect of EECc on histopathological observation of gastric tissue in ketorolac-induced GU rats
Based on histopathological observation of the gastric tissue, the GM surface of the normal group appeared flat and covered with intact epithelium, reflecting a healthy stomach condition (Figure 4(A)). In the negative control group, there was severe GM injury, as seen from extensive epithelial desquamation and the loss of the glandular to submucosal layer. Additionally, there was severe leukocyte infiltration in the lamina propria, indicating an active inflammatory response. The parts showed accumulation of erythrocytes outside the blood vessels, reporting severe bleeding in the GM (Figure 4(B)). The treatment group given OMP showed injury to the GM in the form of minimal desquamation and relatively intact glandular structures, as well as leukocyte infiltration and mild to moderate bleeding seen in several areas (Figure 4(C)). The administration of EECc at all doses showed mild to moderate erosion in the GM. However, the structure remained mostly intact, and necrosis was observed. Mild to moderate leukocyte infiltration appeared in certain areas with bleeding (Figures 4(D) - 4(F)). The histopathological scores of the gastric tissue of rats with ketorolac-induced GU are displayed in Table 4.
Table 4 Effect of EECc on histopathological scoring of gastric tissue in ketorolac-induced GU rats.
The
data are presented as mean ±
SEM (n
= 5).
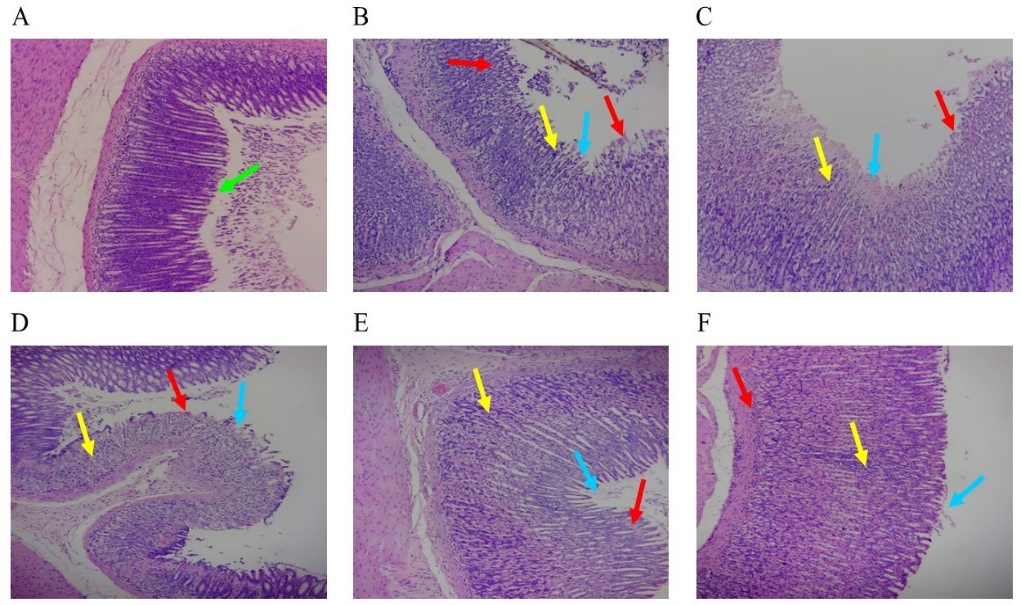
Figure 4 The effect of EECc on histopathological appearance of gastric tissue in ketorolac-induced GU rats. (A) Normal. (B) NC. (C) OMP 20. (D) EECc 50. (E) EECc 100. (F) EECc 200. Light green arrow (gastric mucosa); Light blue arrows (gastric mucosa injury); Yellow arrows (leucocytes infiltration); Red arrows (gastric hemorrhage). Magnification, ×100 and stained with H&E.
Anti-H. pylori activity
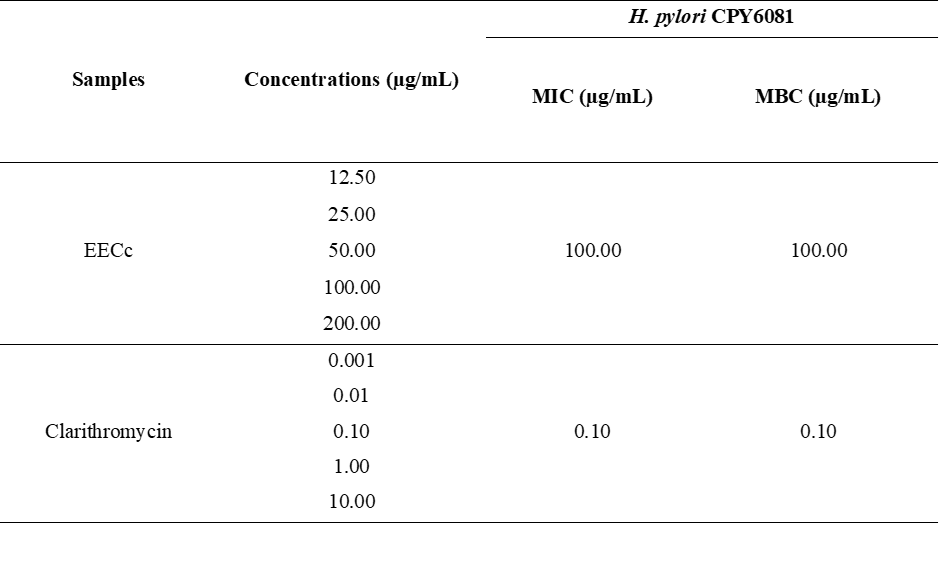
Anti-H. pylori activity of EECc was evaluated by determining MIC and MBC. Based on the results, MIC and MBC of EECc and clarithromycin were 100.00 and 0.10 µg/mL, respectively. Table 5 shows MIC and MBC of EECc and clarithromycin against H. pylori.
Table 5 Determination of MIC and MBC of EECc and clarithromycin against H. pylori CPY6081.
Effect of EECc on gastric juice parameters in H. pylori-induced GU rats
The
induction of
H.
pylori
(1.0×109
CFU) i.g 3 times with an interval of 3 days for 4 weeks, caused an
increase in GpH and GV, as well as a significant decrease in TA (p
< 0.05). Meanwhile, administration of EECc at all doses decreased
(p
< 0.05) the increase in GpH. The EECc 200 also increased (p
< 0.05) the decrease in FA and TA in H.
pylori-induced
GU rats. The administration of TT was reported to have no
significant effect on changes in gastric juice parameters (p
> 0.05) of
H.
pylori-induced
GU rats. The results showed that EECc at all doses, as well as TT,
had a significantly lower UI (p
< 0.001 -
p
< 0.0001) and had inhibition percentages of 28.00%, 45.44%,
67.68%, and 81.13%, respectively. Table
6
shows the effect of EECc administration on gastric juice parameters,
UI, and % inhibition
of ulceration
in
H.
pylori-induced
GU rats.
Table 6 The effect of EECc on GpH, GV, FA, TA, UI, and % inhibition of ulceration in H. pylori-induced GU rats.
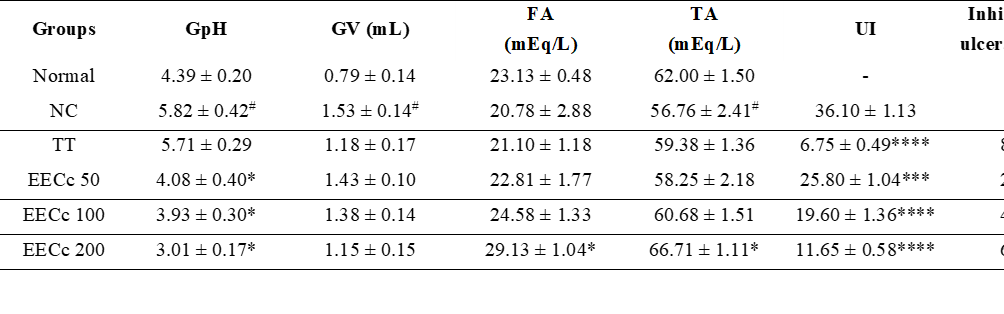
All
experiment data were presented as mean ± SEM (n
= 10 rats). *p
< 0.05, ***p
< 0.001, ****p
< 0.0001 vs. the NC group. #p
< 0.05 vs. the normal group. NC, negative control.
Decrease in H. pylori colonization
Repeated i.g inoculation of H. pylori (1.0×109 CFU/rat) 3 times at 3-day intervals for 4 weeks led to positive reactions in CLO test on the GM. The administration of EECc at all doses over a four-week treatment period showed positive reactions in 70%, 50%, and 30% of the subjects, respectively. Meanwhile, TT reported a positive reaction rate of 10% (Table 7). These results suggested that the TT was more effective in reducing H. pylori colonies in H. pylori-induced GU rats. Repeated i.g. inoculation of H. pylori (1.0×109 CFU/rat) 3 times with an interval of 3 days for 4 weeks increased CLO scores (p < 0.001). Administration of EECc at all doses significantly reduced CLO scores (p < 0.05 - p < 0.01). The results showed that TT administration had a better effect on reducing CLO scores (p < 0.001) in H. pylori-induced GU rats (Figure 5).
Table 7 The effect of EECc on reactivity in the CLO test of gastric mucosa in H. pylori-induced GU rats.
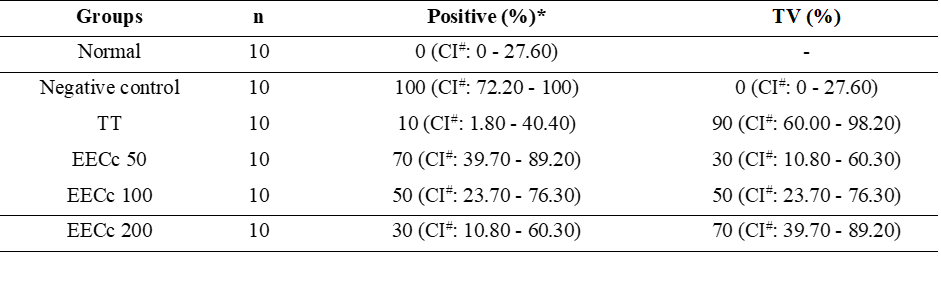
*%
Positive reflects H.
pylori
colonization. #95%
confidential interval (CI). TV, therapeutic
values.
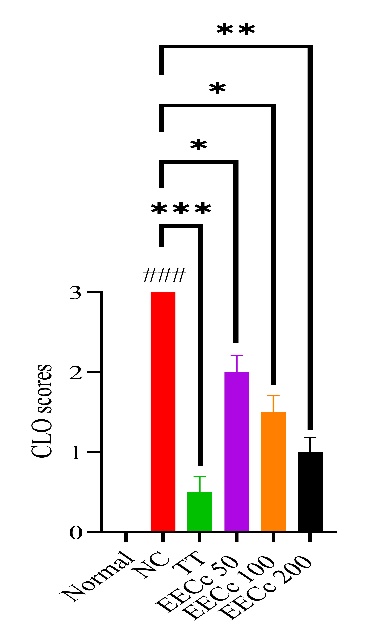
Figure 5 The effect of EECc on CLO scores of GM in H. pylori-induced GU rats. All experiment data were presented as mean ± SEM (n = 10). *p < 0.05, **p < 0.01, ***p < 0.001 vs. the NC group. ###p < 0.001 vs. the normal group. NC, negative control.
Effect of EECc on inflammatory cytokines levels in H. pylori-induced GU rats
Intragastric induction of H. pylori (1.0×109 CFU) 3 times at 3-day intervals for 4 weeks caused a significant increase in TNF-α, IL-1β, IL-6, and PGE2 levels (p < 0.05 - p < 0.0001). Administration of EECc at all doses was reported to significantly decreased the increase in TNF-α (p < 0.05 - p < 0.01), IL-1β (p < 0.05 - p < 0.001), and IL-6 levels (p < 0.05 - p < 0.001) of H. pylori-induced GU rats. Additionally, the EECc 200 reduced PGE2 levels (p < 0.05). Triple therapy did not produce significant changes (p > 0.05) in inflammatory cytokine levels compared to NC. The results suggested that EECc was more effective than TT in modulating inflammatory cytokine levels. Figure 6 shows the effect of EECc on inflammatory cytokine levels in H. pylori-induced GU rats.
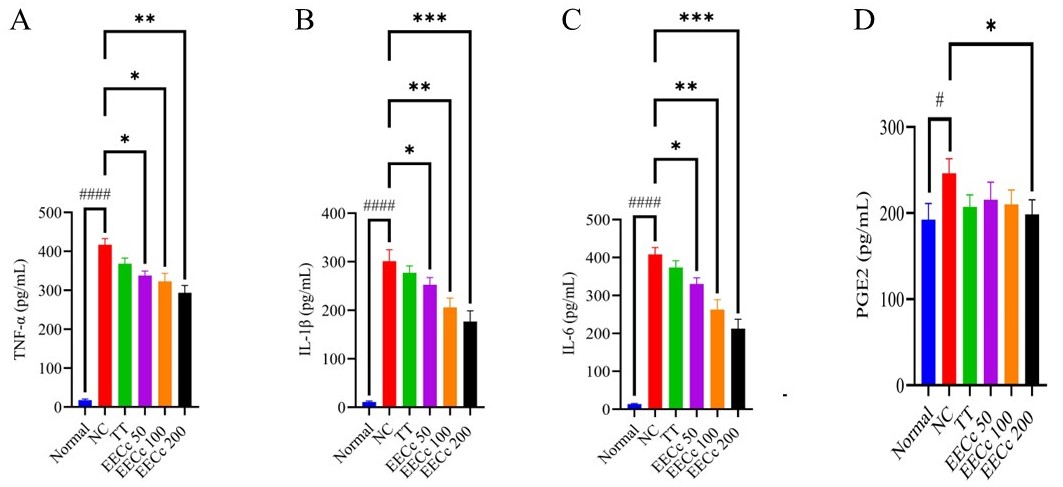
Figure 6 Effect of EECc on inflammatory cytokines levels in H. pylori-induced GU rats. All experiment data were presented as mean ± SEM (n = 10). *p < 0.05, **p < 0.01, ***p < 0.001 vs. the NC group. #p < 0.05-, ####p < 0.0001 vs. the normal group. NC, negative control.
Effect of EECc on histopathological observation of gastric tissue in H. pylori-induced GU rats
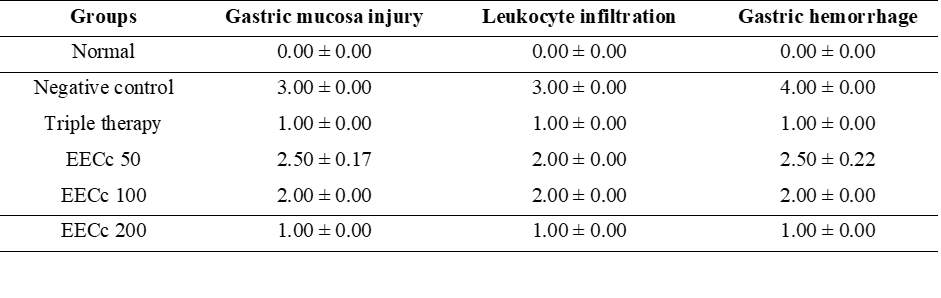
Based on histopathological observation of the gastric tissue, in the normal group, there had been an intact mucosal layer structure and a flat surface covered with a regular epithelial arrangement. There was no desquamation of the gastric glands or visible infiltration of inflammatory cells in the mucosal or submucosal layers, indicating an absence of an inflammatory response. Moreover, no visible bleeding or blood vessel leakage was recorded, as evidenced by the lack of erythrocyte spots outside the vessels (Figure 7(A)). The negative control group showed quite severe GM injury, with damage extending to the middle and lower lamina propria layer. There was also considerable leukocyte infiltration in the lamina propria, with extensive bleeding in the GM (Figure 7(B)). The treatment group given TT reported GM injury characterized by mild desquamation and relatively intact glandular structures, with leukocyte infiltration in only a small area and mild, non-massive bleeding observable in a few regions (Figure 7(C)). Meanwhile, administration of EECc at all doses resulted in mild to moderate GM injury, with preserved structure, necrosis, and leukocyte infiltration confined to a few areas, as well as non-massive bleeding visible in a small area (Figures 7(D) - 7(F)). Table 8 shows the histopathological scores of gastric tissue of H. pylori-induced GU rats.
Table 8 Effect of EECc on histopathological scoring of gastric tissue in H. pylori-induced GU rats.
The
data are presented as mean ±
SEM (n
= 10).
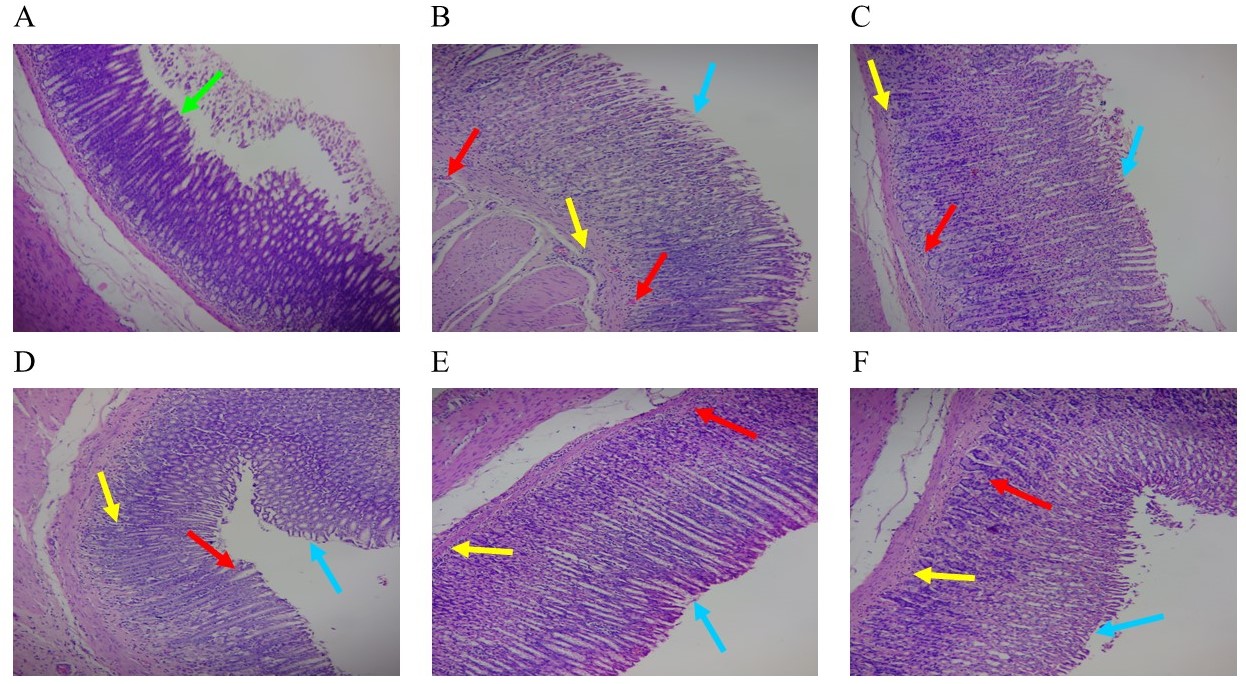
Figure 7 The effect of EECc on histopathological appearance of gastric tissue in H. pylori-induced GU rats. (A) Normal. (B) NC. (C) Triple therapy. (D) EECc 50. (E) EECc 100. (F) EECc 200. Light green arrow (gastric mucosa); Light blue arrows (gastric mucosa injury); Yellow arrows (leucocytes infiltration); Red arrows (gastric hemorrhage). Magnification, ×100 and stained with H&E.
This research assessed antiulcerogenic activity of EECc using EtOH-induced, ketorolac-induced, and H. pylori-induced models of GU. To determine antiulcerogenic effect of EECc, several tests were performed, including measurements of gastric juice parameters, inflammatory cytokine levels, and tissue histopathology. Additionally, in vitro anti-H. pylori activity and in vivo colonization were tested. The administration of 80% EtOH was known to damage rats’ stomach tissue [44]. EtOH quickly penetrated the GM, causing membrane damage, erosion, and cell shedding. These effects led to necrosis and ulcer formation by increasing the permeability of the mucosa to gastric acid and stimulating the production of vasoactive substances by macrophages, as well as mast and blood cells. Moreover, EtOH could affect micro blood vessels by reducing cellular antioxidant levels, disrupting blood flow, and raising inflammatory cytokine production (TNF-α, IL-1β, and IL-6). As a result, the gastric tissue experienced oxidative stress, lipid peroxidation, and hydroperoxyl free radicals, which led to cell death and the development of GU [45,46].
The administration of ketorolac has been reported to cause GU in rats [38]. This GU effect was known because ketorolac increased the production of ROS (superoxide and hydroxyl radicals) and disrupted the defense mechanism of GM by inhibiting prostaglandin production through cyclooxygenase (COX) inhibition [47,48]. Furthermore, ketorolac increased neutrophil adhesion to the blood vessel linings, accompanied by the release of free radicals and protease enzymes in gastric cells [49]. The induction of H. pylori intragastrically for 4 weeks damaged the GM [41]. H. pylori infection, through virulence factors (VacA and CagA), increased ROS formation, promoted the release of inflammatory cytokines, and induced apoptosis of gastric epithelial cells. These effects weakened the GM barrier and increased ulcer formation [50,51].
Measurements of gastric juice parameters with UI were considered to evaluate changes in gastric function caused by ethanol, ketorolac, and H. pylori induction. A decrease in GpH and an increase in GV, FA, TA, and UI were observed in EtOH- and ketorolac-induced GU rats model. In H. pylori-induced GU rats model, there was an increase in GpH and GV, a decrease in FA and TA, and an increase in UI. This occurred because EtOH, ketorolac, and H. pylori damaged the gastric lining, leading to an imbalance between protective and aggressive factors [52-54].
Based on the results, administering EECc 100 and EECc 200 caused a significant increased in the decrease of GpH and decreased the increase in GV, FA, and TA. Meanwhile, EECc 50 decreased the increase in FA and TA. The all doses of EECc were also associated with significantly different UI compared to the NC group in EtOH- and ketorolac-induced GU rats model (Tables 1 and 3). The administration of EECc at all doses significantly decreased the increase in GpH and increased the decrease of FA and TA at EECc 200. EECc at all doses produced a significantly different UI compared to the NC group in H. pylori-induced GU rats model (Table 6). This was due to the strong antioxidant effect of EECc [23,25], which allowed the protection and repair of the GM [55] and gastrin cells (G-cells) to balance protective factors and aggressive in the stomach [56].
The induction of EtOH, ketorolac, and H. pylori increased TNF-α, IL-1β, and IL-6, as well as decreased PGE2 levels (except in the H. pylori-induced GU rats model, there was an increase in PGE2 levels). The administration of EECc at all doses decreased TNF-α, IL-1β, and IL-6, and increased PGE2 levels in EtOH- and ketorolac induced GU rats (Figures 1 and 3), and decreased TNF-α, IL-1β, and IL-6, and decreased PGE2 levels at EECc 200 in H. pylori-induced GU rats (Figure 6). This occured due to anti-inflammatory and antioxidant activities of EECc [25,23], which lowered inflammatory cytokine levels and improved PGE2 levels in the stomachs caused by EtOH, ketorolac, and H. pylori induction. Based on in vitro anti-H. pylori activity testing, EECc had MIC and MBC values of 100.00 µg/mL each against H. pylori growth (Table 5). Meanwhile, in the in vivo anti-H. pylori activity testing, administration of EECc at all doses led to therapeutic effects of 30%, 50%, and 70% in the H. pylori-induced GU rats model (Table 7). Furthermore, EECc at all doses significantly reduced the CLO score (Figure 5). The results were further reinforced by histopathological evidence. In this context, the all doses of EECc improved gastric tissue architecture by reducing the severity of GM injury, decreasing leukocyte infiltration, and minimizing bleeding (Figures 2, 4, and 7). Therefore, the administration of EECc is able to improved and restored the normal functional state of the stomachs in rat models of GU induced by EtOH, ketorolac, and H. pylori, as well as inhibited the growth of H. pylori bacteria. The results of this study are consistent with previous studies which stated that several medicinal plants have anti-ulcerogenic effects in EtOH-, ketorolac-, and H. pylori-induced rat models [36,38,41].
The anti-ulcerogenic effect of EECc is inseparable from its active compounds. Previous research reported that EECc contains 3 kaempferol derivatives, namely kaempferol-3-O-rhamnoside, kaempferol-3-O-α-L arabinoside, and kaempferol-3-O-β-rutinoside [20]. Kaempferol is known to significantly reduce the levels and expression of inflammatory cytokines (TNF-α, IL-1β, and IL-6), inhibits the infiltration and accumulation of neutrophils, and decreases myeloperoxidase (MPO) activity in the gastric tissue. This action helps to control the local inflammatory response that contributes to gastric damage [57]. Additionally, kaempferol can act as a potent antioxidant, directly scavenging ROS and preventing oxidative damage to the GM caused by ulcerogenic substances like ethanol and ketorolac [58]. It also enhances the body’s intrinsic antioxidant defense system by promoting the expression and activity of antioxidant enzymes like superoxide dismutase (SOD) and catalase [59]. On the other hand, kaempferol has been reported to help maintain gastric mucosal glycoproteins and increase NO levels [57]. In cases where GU are caused by bacterial infection, kaempferol can inhibit the growth of H. pylori and reduce the inflammatory process triggered by this bacterium [60,61]. Meanwhile, this study has several limitations, including a sample size that is too small, a limited GU experimental model [absence of other anti-GU tests, such as pyloric ligation-induced GU (pylorus-ligation causes pylorus obstruction which further leads to mucosal digestion as a result of the buildup of pepsin and gastric acid secretion), stress-induced GU (stress-induced GU are sores in the stomach lining that develop rapidly due to severe physical stress, like head injuries/brain trauma, and severe burns), and acetic acid-induced GU in rats], and the absence of in vitro testing [the inhibition of specific enzymes, such as H+/K+-ATPase and gastric cytoprotection (using cell cultures of human gastric epithelial cells)]. Therefore, we recommend future studies to investigate these limitations to improve the evaluation of the efficacy of EECc in GU.
Conclusions
In conclusion, EECc had antiulcerogenic activity in rat GU induced by EtOH, ketorolac, and H. pylori through enhancing gastric function, reducing TNF-α, IL-1β, and IL-6, increasing PGE2 levels, inhibiting H. pylori bacterial growth, and improving gastric tissue structure. Meanwhile, the administration of a dose of 200 mg/kg for 14 days is an estimate of the optimal dose and duration of EECc for the GU model. This promising source of natural compounds was used to develop new antiulcerogenic agents. However, further research could be conducted to understand the exact mechanism of antiulcerogenic effect of EECc.
List of abbreviations
ROS, reactive oxygen species; NSAIDs, nonsteroidal anti-inflammatory drugs; PPIs, proton pump inhibitors; PBS, phosphate buffered saline; TNF-α, tumor necrosis factor-alpha; IL-1β, interleukin-1 beta; IL-6, interleukin-6; ELISA, enzyme-linked immunosorbent assay; ANOVA, analysis of variance; CLSI, clinical and laboratory standards institute; MHB, mueller-hinton broth; V, volume; N, normality; CLA 25, clarithromycin 25 mg/kg; AMOX 50, amoxicillin 50 mg/kg; OMP 20, omeprazole 20 mg/kg; EECc 50, ethanolic extract of Castanopsis costata 50 mg/kg; EECc 100, ethanolic extract of Castanopsis costata 100 mg/kg; EECc 200, ethanolic extract of Castanopsis costata 200 mg/kg; UI, ulcer index; MIC, minimum inhibitory concentration; MBC, minimum bactericidal concentration; CLO, campylobacter-like organism.
Acknowledgements
This research was supported by the Institute for Research and Community Services, Universitas Buana Perjuangan Karawang and Directorate of Research and Community Service, Ministry of Higher Education, Science, and Technology of Indonesia through Regular Fundamental Research (grant no. 0070/C3/AL.04/2025).
Declaration of Generative AI in Scientific Writing
The authors declares that they have not used artificial intelligence (AI)-tools for writing and editing of the manuscript, and no images were manipulated using AI. The authors take full responsibility for the content and conclusions of this work.
CRediT Author Statement
Maulana Yusuf Alkandahri: Conceptualization, Methodology, Supervision, Validation, Funding acquisition, and Writing –original draft preparation. Asman Sadino: Methodology and Visualization. Wilda Fhitriany Usman: Data curation and Validation. Zulpakor Oktoba: Investigation and Visualization. Aprilya Sri Rachmayanti: Data curation and Formal analysis. Rastria Meilanda: Investigation and Formal analysis. Ermi Abriyani: Methodology and Validation. Dani Sujana: Methodology and Formal analysis. Andi Nurzakiah Amal: Writing - Review and Editing. Sigit Roma Rezki Harahap: Investigation and Writing –original draft preparation.
References
[1] M Sharifi-Rad, PVT Fokou, F Sharopov, M Martorell, AO Ademiluyi, J Rajkovic, B Salehi, N Martins, M Iriti and J Sharifi-Rad. Antiulcer agents: From plant extracts to phytochemicals in healing promotion. Molecules 2018; 23(7), 1751.
[2] LL Périco, MT Emílio-Silva, R Ohara, VP Rodrigues, G Bueno, JM Barbosa-Filho, LRMD Rocha, LM Batista and CA Hiruma-Lima. Systematic analysis of monoterpenes: Advances and challenges in the treatment of peptic ulcer diseases. Biomolecules 2020; 10(2), 265.
[3] MA Almadi, Y Lu, AA Alali and AN Barkun. Peptic ulcer disease. Lancet 2024; 404(10447), 68-81.
[4] SS Badapanda, A Kaur, D Jain and D Bhatia. Epidemiology, pathogenesis, and induction of peptic ulcer: A comprehensive review. New Emirates Medical Journal 2024; 5, 1-15.
[5] R Majumder, M Datta, A Banerjee, D Bandyopadhyay and A Chattopadhyay. Melatonin protects against ketorolac induced gastric mucosal toxic injuries through molecular mechanism associated with the modulation of arylakylamine N-acetyltransferase (AANAT) activity. Chemico-Biological Interactions 2023; 382, 110611.
[6] N Vakil. Peptic ulcer disease: A review. JAMA 2024; 332(21), 1832-1842.
[7] R Tan, D Zhao, X Zhang, T Liu, C Han, Z Li, C Qi and Z Wang. Gender and age differences in the global burden of peptic ulcers: An analysis based on GBD data from 1990 to 2021. Frontiers in Medicine 2025; 12, 1586270.
[8] YM Alsinnari, MS Alqarni, M Attar, ZM Bukhari, M Almutairi, FM Baabbad and M Hasosah. Risk factors for recurrence of peptic ulcer disease: A retrospective study in tertiary care referral center. Cureus 2022; 14(2), e22001.
[9] SH Sofi, SM Nuraddin, ZA Amin, HA Al-Bustany and MQ Nadir. Gastroprotective activity of Hypericum perforatum extract in ethanol-induced gastric mucosal injury in wistar rats: A possible involvement of H+/K+ ATPase α inhibition. Heliyon 2020; 6(10), e05249.
[10] O Ahmed, T Nedi and EM Yimer. Evaluation of anti-gastric ulcer activity of aqueous and 80% methanol leaf extracts of Urtica simensis in rats. Metabolism Open 2022; 14, 100172.
[11] YS Kim, HJ Park, H Kim, J Song and D Lee. Gastroprotective effects of Paeonia extract mixture HT074 against experimental gastric ulcers in rats. Evidence-Based Complementary and Alternative Medicine 2019; 2019, 3546258.
[12] AA Calderón-Peña, CL Aspajo-Villalaz, CR Silva-Correa, VET Villarreal-La, MV González-Blas, OE Pretel-Sevillano, ML Salazar-Castillo, M Vaella-Alarcón, F Huaccha-Cáceres, J León-Soto, W Alaya-Davirán, AD González-Siccha, WA Sagástegui-Guarniz, LM Guerrero-Espino and J Hilario-Vargas. Total phenol content and gastric anti-ulcer activity of hydroalcoholic extract of Persea caerulea (Ruiz & Pav.) Mez. Bark. Pharmacognosy Journal 2021; 13(5), 1072-1078.
[13] N Cherrada, AE Chemsa, N Gheraissa, I Laib, Z Gueboudji, M El-Shazly, A Zaater, A Abid, SH Sweilam, TB Emran, S Nani, B Benamor, DG Amara, AV Atoki and M Messaoudi. Gastroprotective efficacy of North African medicinal plants: A review on their therapeutic potential for peptic ulcers. Food Science and Nutrition 2024; 12(11), 8793-8824.
[14] AS Nugraha, RP Agustina, S Mirza, DM Rani, NB Winarto, B Triatmoko, ANW Pratama, PA Keller and P Wangchuk. Phytochemistry and pharmacology of medicinal plants used by the Tenggerese Society in Java Island of Indonesia. Molecules 2022; 27(21), 7532.
[15] MY Alkandahri, YE Maulana, A Subarnas, A Kwarteng and A Berbudi. Antimalarial activity of extract and fractions of Cayratia trifolia (L.) Domin. International Journal of Pharmaceutical Research 2020; 12(S1), 1435-1441.
[16] E Espinoza-Turcios, LI Zambrano, HN Castro-Ramos, J Armada and CR Mejia. Factors associated with the use of medicinal plants for treating diseases and symptoms in Honduras. Journal of Herbs, Spices and Medicinal Plants 2025; 31(1), 38-48.
[17] N Hamzah, Husna, Ruslin and M Arba. The application of medicinal plants in the local community of Gantara Forest, Southeast Sulawesi, Indonesia. Biodiversitas 2022; 23(12), 6557-6563.
[18] TAN Sari, D Nurfitriani, R Mutamimah, Yudianto and AZ Wakhidah. The diversity of medicinal plant used by local community in Borneo, Indonesia: A review. Indonesian Journal of Jamu 2025; 10(1), 24-39.
[19] MY Alkandahri, MG Sholih, NN Fadilah, M Arfania, S Amal, D Frianto, LA Mardiana, D Astuti and DM Hasyim. Evaluation of antidiarrheal, antispasmodic, and antisecretory activities of extract and fractions of Castanopsis costata leaves in animal models. Pharmacognosy Journal 2023; 15(1), 31-37.
[20] MY Alkandahri, A Sadino, WF Usman, E Feriadi, Z Oktoba, AS Ulandari, A Yulyana, A Fathurrohmah, S Khairunnisa, ISA Nisa and AR Salmaduri. Antihyperglycemic and hypoglycemic activities of Castanopsis costata: An experimental study with in vitro, in vivo, and histopathological evaluation. Journal of Applied Pharmaceutical Science 2026; 16(1), 284-295.
[21] MY Alkandahri, A Berbudi, NV Utami and A Subarnas. Antimalarial activity of extract and fractions of Castanopsis costata (Blume) A.DC. Avicenna Journal of Phytomedicine 2019; 9(5), 474-481.
[22] MY Alkandahri, D Sujana, DM Hasyim, MZ Shafirany, L Sulastri, M Arfania, D Frianto, Farhamzah, AH Kusumawati and N Yuniarsih. Antidiabetic activity of extract and fractions of Castanopsis costata leaves on alloxan-induced diabetic mice. Pharmacognosy Journal 2021; 13(S6), 1589-1593.
[23] MY Alkandahri, M Arfania, E Abriyani, D Ridwanuloh, Farhamzah, L Fikayuniar, DM Hasyim, Nurul and D Wardani. Evaluation of antioxidant and antipyretic effects of ethanolic extract of Cep-cepan leaves (Castanopsis costata (Blume) A.DC). Journal of Advanced Pharmacy Education and Research 2022; 12(3), 107-112.
[24] MY Alkandahri, K Kusumiyati, H Renggana, M Arfania, D Frianto, ES Wahyuningsih and YE Maulana. Antihyperlipidemic activity of extract and fractions of Castanopsis costata leaves on rats fed with high cholesterol diet. RASĀYAN Journal of Chemistry 2022; 15(4), 2350-2358.
[25] MY Alkandahri, A Sadino, BT Pamungkas, Z Oktoba, M Arfania, N Yuniarsih, ES Wahyuningsih and DE Putri. Pharmacological evaluation of anti-inflammatory, antipyretic, analgesic, and antioxidant activities of Castanopsis costata leaf fractions (water, ethyl acetate, and n-hexane fractions): The potential medicinal plants from North Sumatra, Indonesia. Research in Pharmaceutical Sciences 2024; 19(3), 251-266.
[26] MY Alkandahri, A Sadino, E Abriyani, F Hermanto, Z Oktoba, MFW Sayoeti, PRA Sangging, D Wardani, N Hasan, SW Sari, NA Safitri, W Ikhtianingsih and S Safitri. Evaluation of hepatoprotective and nephroprotective activities of Castanopsis costata extract in rats. Biomedical Reports 2025; 22(2), 24.
[27] M Beiranvand, S Bahramikia and O Dezfoulian. Evaluation of antioxidant and anti-ulcerogenic effects of Eremurus persicus (Jaub & Spach) Boiss leaf hydroalcoholic extract on ethanol-induced gastric ulcer in rats. Inflammopharmacology 2021; 29(5), 1503-1518.
[28] JDF Rocha, LDC Viana, LCPA Filho, TSD Almeida, JJL Neto, VV Neto, PMS Tabosa, DCS Nunes-Pinheiro, VCC Girão-Carmona, AFU Carvalho and EF Mota. In vitro anti-inflammatory activity and ameliorative effects on gastric ulcers of Licania rigida benth seed extract. Inflammopharmacology 2023; 31(5), 2631-2640.
[29] Z Navvabi, H Anousheh, BJ Kondori, M Ghorbani, M Ghasemi, A Salimi and Z Bahari. Gastroprotective and antioxidant properties of linalyl acetate in ethanol-induced gastric ulcer in rats. Advanced Biomedical Research 2025; 14(1), 49.
[30] NM Alves, PHM Nunes, AM Garcez, MCLD Freitas, IS Oliveira, FVD Silva, HDB Fernandes, DPD Sousa, RDCM Oliveira, DDR Arcanjo and MDCCE Martins. Antioxidant mechanisms underlying the gastroprotective effect of Menthofuran on experimentally induced gastric lesions in rodents. Evidence-Based Complementary and Alternative Medicine 2023; 2023, 9192494.
[31] J Jincy and C Sunil. Exploring antiulcer and anti-inflammatory activities of methanolic leaves extract of an Indian mistletoe Helicantes elasticus (Desv.) Danser. South African Journal of Botany 2020; 133, 10-16.
[32] W Zhang, Y Lian, Q Li, L Sun, R Chen, X Lai, Z Lai, E Yuan and S Sun. Preventative and therapeutic potential of flavonoids in peptic ulcers. Molecules 2020; 25(20), 4626.
[33] CL Venturini, AS Damazo, MJD Silva, JAI Muller, DM Oliveira, FF Figueiredo, BFD Serio, K Arunachalam and DTO Martins. Antiulcer activity and mechanism of action of the hydroethanolic extract of leaves of Terminalia argentea Mart. In different in vivo and in vitro experimental models. Journal of Ethnopharmacology 2024; 318(B), 116972.
[34] C Serafim, ME Araruna, EA Júnior, M Diniz, C Hiruma-Lima and L Batista. A review of the role of flavonoids in peptic ulcer (2010-2020). Molecules 2020; 25(22), 5431.
[35] H Hidayah, S Amal, N Yuniarsih, Farhamzah, AH Kusumawati, NS Gunarti, E Abriyani, ILP Mursal, AK Sundara and MY Alkandahri. Sun protection factor activity of jamblang leaves serum extract (Syzygium cumini). Pharmacognosy Journal 2023; 15(1), 134-140.
[36] AM Mousa, NM El-Sammad, SK Hassan, AENA Madboli, AN Hashim, ES Moustafa, SM Bakry and EA Elsayed. Antiulcerogenic effect of Cuphea ignea extract against ethanol-induced gastric ulcer in rats. BMC Complementary and Alternative Medicine 2019; 19(1), 345.
[37] RN Mohemmad, BS Ahmed, VA Ahmed, SM Ismail and HS Rahman. Anti-inflammatory, antioxidant, and gastro-protective actions of cardamom essential oil-loaded nanostructured lipid carrier in ethanol-induced gastric ulcer. Natural Product Communications 2024; 19(8), 1-10.
[38] AZ Darkazally, A Alnour and S Homsi. Troxerutin effect on gastric ulcers induced by ketorolac in rats: Relation with oxidative stress. Heliyon 2024; 10(19), e38893.
[39] FR Cockerill, MA Wikler, J Alder, MN Dudley, GM Eliopoulos, MJ Ferraro, DJ Hardy, DW Hecht, JA Hindler, JB Patel, M Powell, JM Swenson, RBT Jr, MM Traczewski, JD Turnidge, MP Weinstein and BL Zimmer. Methods for dilution antimicrobial susceptibility tests for bacteria that grow aerobically; Approved standard–ninth edition. Clinical and Laboratory Standards Institute 2012; 32(2), M07-A9.
[40] MM Masadeh, AS Alkofahi, KH Alzoubi, HN Tumah and K Bani-Hani. Anti-Helicobacter pylori activity of some Jordanian medicinal plants. Pharmaceutical Biology 2014; 52(5), 566-569.
[41] MB Santiago, LF Leandro, RB Rosa, MV Silva, SC Teixeira, JPS Servato, SR Ambrósio, RCS Veneziani, JA Aldana-Mejía, JK Bastos and CHG Martins. Brazilian red propolis presents promising anti-H. pylori activity in in vitro and in vivo assays with the ability to modulate the immune response. Molecules 2022; 27(21), 7310.
[42] M Abebaw, B Mishra and DA Gelayee. Evaluation of anti-ulcer activity of the leaf extract of Osyris quadripartite Decne. (Santalaceae) in rats. Journal of Experimental Pharmacology 2017; 9, 1-11.
[43] HM Eltahir. Gastroprotective effect of Quercus infectoria olivier galls on ethanol-induced gastritis in rats. Cureus 2024; 16(3), e56459.
[44] WS Li, SC Lin, CH Chu, YK Chang, X Zhang, CC Lin and YT Tung. The gastroprotective effect of Naringenin against ethanol-induced gastric ulcers in mice through inhibiting oxidative and inflammatory responses. International Journal of Molecular Sciences 2021; 22(21), 11985.
[45] RS El-Shafey, SH Baloza, LA Mohammed, HE Nasr, MM Soliman, HI Ghamry and SA Elgendy. The ameliorative impacts of wheat germ oil against ethanol-induced gastric ulcers: Involvement of anti-inflammatory, antiapoptotic, and antioxidant activities. Toxicology Research 2022; 11(2), 325-338.
[46] MA Ghareeb, HS Mohammed, T Aboushousha, DM Lotfy, MAM El-Shazly, M Sobeh and EFS Taha. Ipomoea carnea mitigates ethanol-induced ulcers in irradiated rats via Nrf2/HO-1 pathway: An in vivo and in silico study. Scientific Reports 2024; 14(1), 3469.
[47] C Musumba, DM Pritchard and M Pirmohamed. Review article: Cellular and molecular mechanisms of NSAID-induced peptic ulcers. Alimentary Pharmacology and Therapeutics 2009; 30(6), 517-531.
[48] SC Park, HJ Chun, CD Kang and D Sul. Prevention and management of non-steroidal anti-inflammatory drugs-induced small intestinal injury. World Journal of Gastroenterology 2011; 17(42), 4647-4653.
[49] JL Wallace. Pathogenesis of NSAID-induced gastroduodenal mucosal injury. Best Practice and Research. Clinical Gastroenterology 2001; 15(5), 691-703.
[50] Rakesh, SD Munjal, RS Sengar, N Sharma, S Rautela and M Singh. Molecular mechanisms of Helicobacter pylori infection: A review. Journal of Pure and Applied Microbiology 2025; 19(3), 1755-1770.
[51] Y Li, G Liu, L Zhou, Y Wang, Y Sun, Y Chen, L Chen and J Xiao. Helicobacter pylori-induced apoptosis in gastric diseases: Mechanisms, implications, and diagnostic applications. International Journal of General Medicine 2025; 18, 2995-3009.
[52] M Raish, M Shahid, YAB Jardan, MA Ansari, KM Alkharfy, A Ahad, IA Abdelrahman, A Ahmad and FI Al-Jenoobi. Gastroprotective effect of sinapic acid on ethanol-induced gastric ulcers in rats: Involvement of Nrf2/HO-1 and NF-κB signaling and antiapoptotic role. Frontiers in Pharmacology 2021; 12, 622815.
[53] L Hong, L Fangqun, Z Chaohui and Z Hengbei. Peptic ulcer and hemorrhagic shock induced by ketorolac tromethamine injection. Adverse Drug Reactions Journal 2022; 24(6), 324-326.
[54] A Ali and KI AlHussaini. Helicobacter pylori: A contemporary perspective on pathogenesis, diagnosis and treatment strategies. Microorganisms 2024; 12(1), 222.
[55] F Zhu, H Pan, B Li, X Mao, Z Chen, G Ye, J Gao, Y Shen, J Hu and Z Lou. Hericium erinaceus extract attenuates gastric mucosal injury via Nrf2/HO-1 pathway activation and gut microbiota modulation in rats. Journal of Functional Foods 2025; 128, 106842.
[56] JL MacNicol and W Pearson. Gastrin and nitric oxide production in cultured gastric antral mucosa are altered in response to a gastric digest of a dietary supplement. Frontiers in Veterinary Science 2021; 8, 684203.
[57] Q Li, X Hu, Y Xuan, J Ying, Y Fei, J Rong, Y Zhang, J Zhang, C Liu and Z Liu. Kaempferol protects ethanol-induced gastric ulcers in mice via pro-inflammatory cytokines and NO. Acta Biochimica et Biophysica Sinica 2018; 50(3), 246-253.
[58] H Liu, Y Chen, Y Hu, W Zhang, H Zhang, T Su, J Wang, Z Yin, X Zhao, X Zhou, L Li, Y Zou, Y Fu, Y Zhang and X Song. Protective effects of an alcoholic extract of Kaempferia galanga L. rhizome on ethanol-induced gastric ulcer in mice. Journal of Ethnopharmacology 2024; 325, 117845.
[59] F Alrumaihi, SA Almatroodi, HOA Alharbi, WM Alwanian, FA Alharbi, A Almatroudi and AH Rahmani. Pharmacological potential of kaempferol, a flavonoid in the management of pathogenesis via modulation of inflammation and other biological activities. Molecules 2024; 29(9), 2007.
[60] R Yang, J Li, J Wang, Y Wang, F Ma, R Zhai and P Li. Kaempferol inhibits the growth of Helicobacter pylori in a manner distinct from antibiotics. Journal of Food Biochemistry 2022; 46(9), e14210.
[61] MJ Yeon, MH Lee, DH Kim, JY Yang, HJ Woo, HJ Kwon, C Moon, SH Kim and JB Kim. Anti-inflammatory effects of kaempferol on Helicobacter pylori-induced inflammation. Bioscience, Biotechnology, and Biochemistry 2019; 83(1), 166-173.