Trends
Sci.
2026;
23(10):
13261
Effect of Pomegranate (Punica Granatum L.) Extract on Endothelial Dysfunction, Vascular, and Renal Damage in a Rat Model of Preeclampsia
Endang
Sri
Wahyuni1,8,
![]() ,
Soetrisno1,2,
,
Soetrisno1,2,
![]() ,
Bambang Purwanto1,3,
,
Bambang Purwanto1,3,
![]() ,
Brian Wasita1,4,*,
,
Brian Wasita1,4,*,
Vitri
Widyaningsih1,5,
![]() ,
Risya Cilmiaty1,6,
,
Risya Cilmiaty1,6,
![]() and Paramasari Dirgahayu1,7,
and Paramasari Dirgahayu1,7,
![]()
1Doctoral Program of Medical Sciences, Faculty of Medicine, Universitas Sebelas Maret, Surakarta 57126, Indonesia
2Department of Obstetrics and Gynaecology, Faculty of Medicine, Universitas Sebelas Maret,
Surakarta 57126, Indonesia
3Department of Internal Medicine, Faculty of Medicine, Universitas Sebelas Maret, Surakarta 57126, Indonesia
4Department of Anatomical Pathology, Faculty of Medicine, Universitas Sebelas Maret, Surakarta 57126, Indonesia
5Department of Public Health, Faculty of Medicine, Universitas Sebelas Maret, Surakarta 57126, Indonesia
6Department of Oral Disease, Faculty of Medicine, UNS Hospital, Universitas Sebelas Maret,
Surakarta 57126, Indonesia
7Departement of Parasitology Faculty of Medicine, Universitas Sebelas Maret, Surakarta 57126, Indonesia
8Departement of Midwifery, Faculty of Health Sciences, Universitas ‘Aisyiyah Surakarta, Surakarta 57146, Indonesia
(*Corresponding author’s e-mail: [email protected])
Received: 4 January 2026, Revised: 10 March 2026, Accepted: 17 March 2026, Published: 10 May 2026
Abstract
Preeclampsia is a hypertensive disorder of pregnancy marked by elevated blood pressure, proteinuria, and involvement of multiple maternal organs, posing substantial risks to both mother and fetus. Existing therapeutic approaches mainly focus on symptom control and do not directly address the underlying pathophysiological disturbances. This study investigated the potential protective effects of pomegranate (Punica granatum L.) extract in an L-NAME–induced rat model of preeclampsia. Pregnant Sprague-Dawley rats were allocated into 5 experimental groups: Normal pregnancy control, L-NAME–induced preeclampsia (75 mg/kgBW/day), preeclampsia treated with magnesium sulfate (MgSO₄), preeclampsia treated with pomegranate extract (500 mg/kgBW/day), and combination therapy. Biomarkers of oxidative stress (MDA), inflammatory activation (NF-κB), endothelial function (NO), placental vascular remodeling (spiral artery diameter), renal injury (KIM-1), as well as blood pressure, proteinuria, and fetal weight were evaluated. Administration of pomegranate extract significantly lowered NF-κB levels and enhanced nitric oxide availability compared with untreated preeclamptic rats, suggesting reduced inflammatory signaling and improved endothelial performance. Although MDA values tended to decrease in treated groups, this change did not reach statistical significance. The intervention was also associated with enlargement of spiral artery diameter, reduction in KIM-1 expression, slower progression of hypertension and proteinuria, and improved fetal growth. Combined treatment with magnesium sulfate showed additional benefits in several vascular and renal parameters. Overall, these findings indicate that pomegranate extract may exert broad protective effects in experimental preeclampsia by influencing interconnected inflammatory and endothelial pathways, supporting vascular remodeling and renal preservation. The results highlight its potential as an adjunct therapeutic candidate aimed at improving maternal vascular function and fetal development.
Keywords: Preeclampsia, Pomegranate extract, Oxidative stress, Inflammation, Nitric oxide, NF-κB, MDA, KIM-1
Introduction
Preeclampsia is one of the most dangerous conditions during pregnancy, impacting the health of both mother and fetus. Preeclampsia is characterized by increased blood pressure, proteinuria, and damage to vital organs such as the kidneys and placenta that occurs after 20 weeks of gestation. At the molecular level, preeclampsia is strongly associated with endothelial dysfunction driven by excessive oxidative stress and systemic inflammation. Preeclampsia affects approximately 2% - 8% of all pregnancies and is a major cause of maternal and perinatal morbidity and mortality worldwide [1-3]. Although there has been extensive research examining the causes and management of preeclampsia, so far existing treatments are still limited to managing symptoms, and have not been able to address the underlying causes, namely endothelial dysfunction and vascular disorders caused by oxidative stress, and systemic inflammation [4,5].
Oxidative stress is a central mechanism in the pathogenesis of preeclampsia. Excessive production of reactive oxygen species promotes endothelial injury, increases vascular permeability, and aggravates vascular and renal dysfunction. One consequence of this process is lipid peroxidation, which can be reflected by malondialdehyde (MDA) as a marker of oxidative damage [6-8].
One of the hallmarks of preeclampsia is a failure of placental vascular remodeling. The spiral arteries, which should dilate to reduce vascular resistance, instead constrict, increasing resistance and causing placental ischemia [9]. This reduces fetal blood supply, which can lead to impaired fetal growth. Furthermore, increased levels of reactive oxygen species (ROS) inhibit the production of nitric oxide (NO), which functions as a vasodilator and is essential for maintaining vascular tone [10]. Decreased NO is associated with impaired vasodilation, which worsens hypertension and vascular dysfunction in the placenta and kidneys [11,12].
Despite advances in understanding its pathophysiology, current management of preeclampsia remains largely symptomatic. Magnesium sulfate is effective for seizure prophylaxis, but it does not directly target oxidative stress, endothelial dysfunction, or placental vascular remodeling. Therefore, identifying adjunct therapies that address these underlying mechanisms is of considerable clinical interest. With limited therapeutic options available, increasing attention is being paid to plant-based therapies as a promising alternative. Plant-derived polyphenols have gained attention for their antioxidant, anti-inflammatory, and vasculoprotective properties [13-15]. One potential candidate is pomegranate (Punica granatum L.) extract, which is rich in bioactive compounds such as polyphenols and flavonoids, known to have antioxidant, anti-inflammatory, and antihypertensive effects. Several previous studies have shown that pomegranate extract can reduce oxidative stress, lower blood pressure, and improve endothelial function, suggesting its potential in addressing vascular dysfunction and inflammation in preeclampsia [13,14].
Although previous studies have demonstrated the antioxidant and antihypertensive effects of pomegranate extract, most investigations have focused on isolated parameters such as blood pressure or oxidative markers. Comprehensive evaluation of its effects on endothelial dysfunction, placental vascular remodeling, renal injury markers (KIM-1), and fetal growth in a preeclampsia model remains limited. Thus, a critical gap persists regarding whether pomegranate extract can exert integrated multi-target protective effects on oxidative stress, inflammation, vascular remodeling, renal damage, and fetal outcomes in preeclampsia. We hypothesized that pomegranate extract would attenuate oxidative stress and inflammatory activation, restore nitric oxide bioavailability, improve spiral artery remodeling, reduce renal injury, and ultimately enhance fetal growth in an L-NAME-induced rat model of preeclampsia. This study was therefore designed to evaluate the effects of pomegranate extract on MDA, NF-κB, NO levels, spiral artery diameter, KIM-1 expression, blood pressure, proteinuria, and fetal weight in a controlled experimental model of preeclampsia.
Materials and methods
Chemicals
N-omega-Nitro-L-arginine Methyl Ester Hydrochloride (L-NAME; CAS No. 51298-62-5), and magnesium sulfate ( MgSO4; Catalog No. NL0020) was purchased from Tokyo Chemical Industry Co., Ltd. (Tokyo, Japan). ELISA kits for rat malondialdehyde (MDA; Cat. No. E0156Ra), nuclear factor-κB (NF-κB; Cat. No. E0287Ra), and nitric oxide (NO; Cat. No. E0703Ra) were obtained from Bioassay Technology Laboratory (Zhejiang, China). Polyclonal anti-kidney injury molecule-1 (KIM-1; Cat. No. PAA785Ra01) antibody was purchased from Sigma-Aldrich (St. Louis, MO, USA).
Collection of plant materials and preparation of extracts
The fruit samples were sourced from a pomegranate orchard in Situbondo, East Java, Indonesia. The specimens were identified and confirmed by the Functional Implementation Unit of the Tawangmangu Traditional Health Service at Dr. Sardjito General Hospital (certification no. TL.02.04/D.XI.6/24934.1145/2024). The pomegranates were rinsed with distilled water to eliminate contaminants and then dried in an oven at 50 °C for 72 h. After drying, the fruit was ground into a fine powder and sieved using a 60-mesh screen. The extraction process utilized the maceration method, combining the pomegranate powder with 70% (v/v) ethanol and stirring occasionally to ensure uniform mixture. This mixture was left to macerate for 120 h at room temperature (24 ± 2 °C) within a closed container to shield it from light. Following this, the mixture was filtered using vacuum filtration with Whatman No. 1, and the ethanol solvent was removed using a rotary evaporator, resulting in a concentrated extract. The extract was then dried at 40 °C until it reached a constant weight, producing a thick paste that is ready for use.
Experimental design
The experimental procedure was approved and conducted under the supervision of the Ethical Clearance Commission for preclinical research of the Integrated Research and Testing Laboratory of Universitas Gadjah Mada (No.: 00006/II/UN1/LPPT/EC/2025). Healthy female Sprague Dawley rats aged 8 - 10 weeks weighing 180 - 250 g were mated with male rats aged 8 - 12 weeks weighing 250 - 350 g. Pregnancy was determined from the results of vaginal smears that found sperm, then defined as day 0 of pregnancy . Then the smear was observed under an XSP 13A microscope at 100x magnification. Preeclampsia induction was carried out by intraperitoneal injection of 75 mg/kgBW/day of L-NAME from the 9th to the 19th day of pregnancy. L-NAME inhibits NO synthesis, which leads to increased blood pressure and impaired blood flow, which are the main characteristics of preeclampsia. Rats were randomly assigned (n = 7 per group) to 5 groups: 1. Normal pregnant control NG; 2. Preeclampsia + L-NAME as negative control group C(‒); 3. Preeclampsia + MgSO₄ (120 mg/kg, intraperitoneally on GD 18 - 19) as positive control group C(+); 4. Preeclampsia + pomegranate extract (500 mg/kg/day, GD 9 - 19) as treatment group T1; 5. Preeclampsia + MgSO₄ + pomegranate extract as combination treatment group T2.
All rats were maintained in a controlled environment with a temperature of 24 ± 2 °C, humidity of 40% - 60%, and a 12-hour day and 12-hour night lighting cycle. Food and water were freely provided, and rats were given 1 week to adapt before treatment began. At the end of the experimental period, all animals were sacrificed using 90 - 100 mg/kg ketamine and 10 mg/kg xylazine intramuscularly or intraperitoneally (cervical dislocation was performed to verify mouse mortality).
Measurement of blood pressure and urine protein
The pressure measurement instrument uses the CODA Non-invasive blood pressure system from Kent Scientific. This examination involves inserting the ratʼs tail into a special cuff (Cuff Occlusion and VPR Cuff) sequentially, then connecting the cuff to the CODA controller, and running software on a computer for installation and blood pressure measurement (Systolic & Diastolic), using Volume Pressure Recording (VPR) technology. This system will measure systolic and diastolic blood pressure automatically. Rat urine was collected by placing it in a separate metabolic cage for 24 h. Urine protein concentration was detected using the biuret method. Urine samples were centrifuged to remove particles, followed by mixing with Biuret reagent. The solution was conditioned at room temperature for 10 - 30 min to develop color. Absorbance was measured at 540 nm using a spectrophotometer. The absorbance value was correlated with a standard calibration curve to determine protein levels. Blood pressure and urine protein Measurements were performed on gestational day (GD) 8, 12, 16, and 19.
Measurement of oxidative stress levels, inflammation and vasodilatory capacity and vascular function in the placenta
Placental tissues were homogenized and analyzed for MDA, NF-κB, and NO levels using ELISA kits according to the manufacturers’ protocols. Concentrations were expressed as nmol/mL tissue (MDA), ng/mL (NF-κB), and µmol/L (NO). Placental tissue was fixed in 10% neutral buffered formalin overnight, washed in PBS, and embedded in paraffin for 5 μM sectioning. Sections were deparaffinized in xylene and rehydrated through decreasing ethanol concentrations before hematoxylin and eosin staining. After dehydration, embedding, and sectioning, H&E staining was performed for observation.
Histopathological analysis
Placental tissues were fixed in 10% neutral buffered formalin, embedded in paraffin, and sectioned at 5 µm thickness. Sections were deparaffinized, rehydrated, and stained with hematoxylin and eosin (H&E). Spiral artery diameter was measured under light microscopy at 200x magnification using calibrated imaging software.
Immunohistochemical analysis of KIM-1
Kidney tissue from rats as samples was prepared for the IHC preparation process. It began with cutting the paraffin block into 4 - 5 micron slices, placed on poly-L-lysine slides and incubated at 37 °C overnight. The deparaffinization process was carried out by successive immersion in xylene and alcohol, ending with aquadest washing. Antigen retrieval was performed using a microwave with Tris EDTA pH 9, followed by washing with PBS. Endogenous peroxidase was inhibited using 3% methanol H₂O₂. Next, the slices were dropped with blocking serum and specific antibodies, incubated at 4 °C overnight. After washing, biotin and streptavidin were added. DAB as a peroxidase enzyme substrate was added before washing with running water and staining with hematoxylin. The preparations were then mounted and covered with a coverslip. KIM-1 expression was semi-quantitatively analyzed.
Fetal weight measurement
On GD 20, fetuses were delivered by cesarean section and individually weighed using a calibrated digital balance (Mettler Toledo, USA). The number of fetuses and their respective weights were recorded, then mean fetal weight per mg was calculated.
Statistical analysis
Data are presented as mean ± standard deviation (SD). Normality was assessed using the Shapiro-Wilk test, and homogeneity of variance was assessed using Levene’s test. For normally distributed variables with homogeneous variance, one-way analysis of variance (ANOVA) followed by Tukey’s honestly significant difference (HSD) post hoc test was used. When variance heterogeneity was present, Welch’s ANOVA followed by Games-Howell post hoc testing was applied. Non-normally distributed variables were analyzed using the Kruskal-Wallis test followed by adjusted pairwise comparisons. Repeated-measures ANOVA was used to evaluate longitudinal changes in blood pressure and proteinuria, including time, group, and time×group interaction effects. When sphericity assumptions were violated, corrected estimates were applied. Log10 transformation was used when required to improve distributional assumptions. Statistical significance was defined as p < 0.05. All analyses were performed using IBM SPSS Statistics version 25 (IBM Corp., USA).
Ethical considerations
The research involving plant material was approved by the Ethics Committee of Universitas Gadjah Mada, Yogyakarta, Indonesia, (certification no. 00006/II/UN1/LPPT/EC/2025).
Results and discussion
The present study demonstrates that pomegranate extract exerts integrated protective effects in an L-NAME-induced rat model of preeclampsia. The intervention modulated inflammatory signaling, improved nitric oxide bioavailability, attenuated renal injury, and enhanced placental vascular remodeling, collectively contributing to improved maternal and fetal outcomes.
Effects of pomegranate extract on oxidative stress (MDA)
Malondialdehyde (MDA) was measured as an index of lipid peroxidation and oxidative stress. As presented in Table 1(A), the untreated preeclampsia group showed the highest mean MDA level (2.34 ± 0.10), whereas the normal pregnancy group showed the lowest level (1.91 ± 0.10). Because variance heterogeneity was observed, group differences were evaluated using Welch’s ANOVA, which did not indicate a significant overall group effect F(4, 14.697) = 2.024, p = 0.144. Consistently, Games-Howell post hoc testing showed no significant pairwise differences (all adjusted p > 0.05), with the largest mean difference observed between the normal pregnancy and untreated preeclampsia groups (adjusted p = 0.069).
All treated groups (MgSO₄, pomegranate extract, and combination therapy) showed lower mean MDA levels compared with the untreated preeclampsia group (Table 1(A); Figure 1(A)). However, pairwise comparisons did not demonstrate statistically significant differences between the untreated preeclampsia group and each treated group. Therefore, the reductions observed in the treated groups should be interpreted as a downward trend rather than a confirmed statistically significant decrease.
Oxidative stress plays a central role in the pathogenesis of preeclampsia. Excessive reactive oxygen species (ROS) production promotes lipid peroxidation, endothelial injury, and reduced nitric oxide bioavailability, ultimately contributing to vascular dysfunction and hypertension [5]. In this context, the downward trend in MDA levels in the pomegranate-treated groups may be biologically plausible. Experimental studies have demonstrated that pomegranate extract can attenuate lipid peroxidation and modulate endothelial oxidative responses in preeclampsia-related models [15,16]. The antioxidant properties of pomegranate are largely attributed to its polyphenolic constituents, including punicalagin and ellagic acid, which exhibit free radical scavenging activity [17].
Although the reduction in MDA did not reach statistical significance in pairwise post hoc testing, the overall pattern supports a potential antioxidant effect that may contribute to downstream improvements in inflammatory activation and endothelial function. The results of this study are consistent with previous studies showing that pomegranate extract can reduce oxidative stress and improve vascular function in preeclampsia, as reported by Nasifah who found a decrease in MDA and improved vascular function with pomegranate extract administration [16]. Pomegranate extract has a significant antioxidant effect, which contributes to reducing lipid peroxidation and improving vascular health in pregnancy-related hypertension conditions [18]. A study conducted by Hosry also showed that the phenolic content of pomegranate can reduce cell damage caused by oxidative stress and inflammation, which play an important role in the pathogenesis of preeclampsia [17]. Oxidative stress plays an important role in the development of preeclampsia, as described in the literature. The role of Reactive Oxygen Species (ROS) in damaging cellular structures, including damage to DNA, lipids, and proteins, can cause disruption to maternal and fetal organ function. In this study, the downward trend in MDA levels suggests a possible modulation of oxidative stress, although this effect was not statistically significant [19,20].
Effect of pomegranate extract on inflammatory activation (NF-κB)
NF-κB is a pivotal transcription factor regulating pro-inflammatory cytokines, adhesion molecules, and oxidative pathways implicated in endothelial dysfunction during preeclampsia. Persistent NF-κB activation amplifies systemic inflammation and contributes to vascular injury [21,22]. NF-κB levels were evaluated to assess inflammatory activation in the L-NAME-induced preeclampsia model. As shown in Table 1(B), NF-κB levels differed significantly among groups (one-way ANOVA, p < 0.001). The untreated preeclampsia group showed the highest NF-κB level (3.84 ± 0.30 ng/mL), whereas the normal pregnancy group showed the lowest level (2.98 ± 0.24 ng/mL). Tukey HSD post hoc analysis demonstrated that the untreated preeclampsia group had significantly higher NF-κB levels than the normal pregnancy group (p < 0.001), the pomegranate-treated group (p = 0.040), and the combination group (p = 0.021). The normal pregnancy group also differed significantly from the MgSO₄ group (p < 0.001), the pomegranate-treated group (p = 0.019), and the combination group (p = 0.035), whereas no significant difference was observed between the pomegranate-treated and combination groups.
As illustrated in Figure 1(B), administration of pomegranate extract, either alone or in combination with MgSO₄, shifted NF-κB levels toward the normal range. These findings suggest that pomegranate extract attenuated inflammatory activation in experimental preeclampsia. This interpretation is biologically plausible because NF-κB is a key transcription factor involved in the regulation of inflammatory cytokines, adhesion molecules, and endothelial injury in preeclampsia [5,17,21,22]. Previous studies have also shown that pomegranate-derived polyphenols, including punicalagin and ellagic acid, can suppress NF-κB signaling and reduce inflammatory mediator expression [23-28]. Collectively, these findings support the anti-inflammatory potential of pomegranate extract in this model.
Effect of pomegranate extract on nitric oxide (NO)
Nitric oxide (NO) levels were measured to evaluate endothelial function in the L-NAME-induced preeclampsia model. As presented in Table 1(C), NO levels differed significantly among groups (one-way ANOVA, p < 0.001). The untreated preeclampsia group exhibited the lowest NO level (76.57 ± 7.60 µmol/L), whereas the normal pregnancy group showed a higher level (93.50 ± 5.69 µmol/L). Tukey HSD post hoc analysis showed that the untreated preeclampsia group had significantly lower NO levels than the normal pregnancy group (p = 0.003), the MgSO₄ group (p = 0.016), the pomegranate-treated group (p < 0.001), and the combination group (p = 0.011). In addition, the pomegranate-treated group had significantly higher NO levels than the MgSO₄ group (p = 0.018) and the combination group (p = 0.025).
As shown in Figure 1(C), treatment with pomegranate extract increased NO levels relative to the untreated preeclampsia group, indicating improvement of endothelial function. Reduced NO bioavailability is a well-recognized feature of preeclampsia and contributes to vasoconstriction, hypertension, and impaired uteroplacental perfusion [5,29,30]. The restoration of NO observed in the treated groups may reflect improved endothelial nitric oxide balance, potentially mediated by reduced inflammatory activation and improved oxidative status. These results are consistent with previous reports suggesting that pomegranate extract can support endothelial function and nitric oxide-related vascular responses [16,29,31,32].
Table 1 Differences in MDA, NF-κB, NO levels, spiral artery diameter, KIM-1 expression in preeclampsia rat models given pomegranate extract.
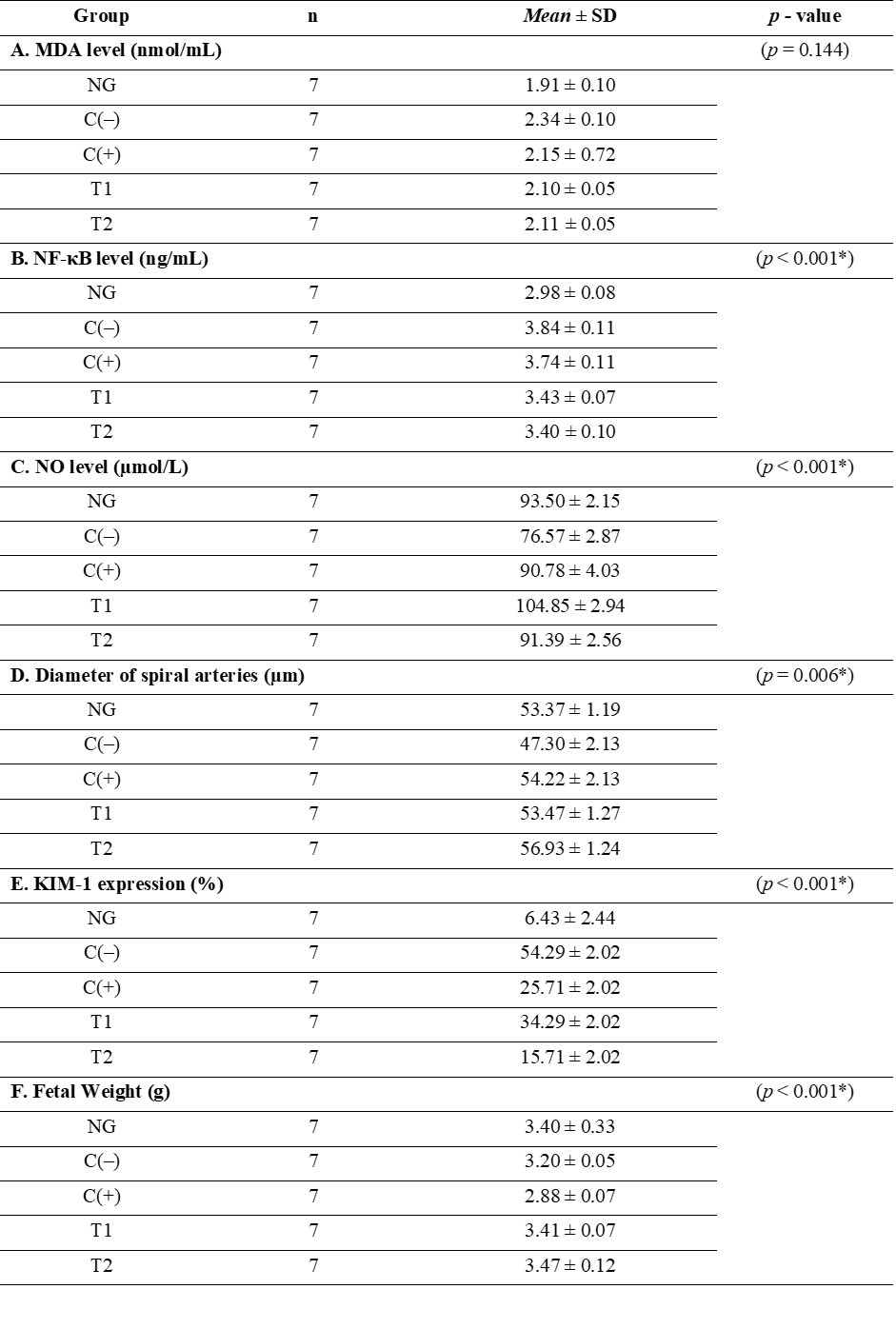
Description: NG = Normal pregnant rats, C(‒) = Pregnant rats induced by L-NAME 75 mg/kgBW/day. C(+) = Pregnant rats induced by L-NAME treated with standard MgSO4 (120 mg/kg), T1 = Pregnant rats induced by L-NAME treated with pomegranate extract 500 mg/kgBW, T2 = Pregnant rats induced by L-NAME treated with standard MgSO4 (120 mg/kg) and pomegranate extract 500 mg/kgBW/day.
Figure 1 Effect of pomegranate extract on placental and renal outcome markers in the rat model of preeclampsia. (A) MDA level, (B) NF-κB level, (C) NO level, (D) Spiral artery diameter, (E) KIM-1 expression, and (F) Fetal weight. Data are presented as mean ± SD. Statistical significance was set at p < 0.05.
Effect of pomegranate extract on diameter spiral artery
Spiral artery diameter measurements were used to evaluate the effect of pomegranate extract on the structural changes of blood vessels in the placenta in a preeclampsia model. In preeclampsia, there is a disruption in the formation and remodeling of placental blood vessels, which causes narrowing of the spiral arteries and reduced blood flow to the placenta, increasing the risk of complications for the mother and fetus [35-37]. In Table 1(D), spiral artery diameter differed significantly among groups (one-way ANOVA, p = 0.005). Tukey HSD post hoc analysis showed that the untreated preeclampsia group had a significantly smaller spiral artery diameter than the MgSO₄ group (p = 0.043) and the combination group (p = 0.002). The difference between the untreated preeclampsia group and the pomegranate-treated group approached significance (p = 0.088), while no significant difference was observed between the normal pregnancy and treatment groups. This indicates that standard therapy can reduce preeclampsia symptoms, but does not completely improve the vascular disorders that occur. In the T1 group, the spiral artery diameter increased to (53.47 ± 1.27 µm). This increase in diameter indicates that pomegranate extract, which is rich in bioactive compounds such as flavonoids and ellagic acid, has a vasoprotective effect that can improve vascular endothelial function and help improve the diameter of narrowed spiral arteries in preeclampsia. The T2 group showed a greater increase in spiral artery diameter (56.93 ± 1.24 µm) compared to the C(‒) and C(+) groups (Figures 1(D) and 2(E)). These results indicate that the combination of these 2 therapies provides a synergistic effect in enhancing blood vessel remodeling, increasing blood flow to the placenta, and improving the supply of oxygen and nutrients needed by the fetus.
Structural evaluation further strengthens the functional findings. Impaired spiral artery remodeling is a defining feature of preeclampsia, leading to increased placental vascular resistance and compromised fetal perfusion. The significant increase in spiral artery diameter in pomegranate-treated groups suggests improved placental vascular adaptation. The more pronounced effect observed in the combination therapy group may indicate additive or synergistic mechanisms between magnesium sulfate and pomegranate extract [20,27,38,39].
Figure 2 Effect of pomegranate extract administration on the diameter of the placental artery lumen. Histopathological analysis of placental tissue from: (A) normal pregnancy group, (B) preeclampsia group, (C) preeclampsia group treated with standard drugs, (D) preeclampsia group treated with pomegranate extract, and (E) the preeclampsia group treated with standard therapy combined with pomegranate extract. Hematoxylin and eosin (H&E) staining showed a decrease in diameter in the preeclampsia group (B), and an increase in diameter in the treated group. Images were taken at 200x magnification (20x objective lens, 10x ocular lens).
Effect of pomegranate extract on KIM-1 expression
Kruskal-Wallis analysis showed a significant difference in KIM-1 expression among groups (p < 0.001). Post hoc pairwise comparisons with Bonferroni adjustment revealed that the untreated preeclampsia group differed significantly from the normal pregnancy group p < 0.001 and from the T2 group p = 0.001. In addition, the normal pregnancy group differed significantly from the T1 group p = 0.003. No other pairwise comparisons reached statistical significance.
KIM-1 expression measurements were performed to evaluate kidney damage in the preeclampsia model. In Table 1(E), the NG group showed low KIM-1 expression (6.43 ± 2.44%), reflecting normal kidney function. In the C(‒) group, KIM-1 expression increased significantly (54.29 ± 2.02%), indicating kidney damage caused by oxidative stress and inflammation, consistent with previous findings showing increased KIM-1 expression in preeclampsia models [23,24,38]. The C(+) group showed a decrease in KIM-1 expression, although not significant compared to the PE group p = 0.111. This indicates that although standard therapy can reduce hypertension symptoms in preeclampsia, its effect on kidney damage is still limited. The decrease in KIM-1 expression in the T1 group indicates that pomegranate extract has the potential to protect the kidneys by reducing oxidative stress and inflammation, which is in line with studies showing that pomegranate extract can improve kidney function in inflammatory conditions [26,27]. The T2 group showed a more significant decrease in KIM-1 expression (15.71 ± 2.02%), which reflects the synergistic effect of these 2 therapies in repairing kidney damage that occurs due to preeclampsia (Figures 1(E) and 3(E)). This decrease is also in accordance with studies showing that combination therapy can increase organ protection, especially the kidneys, in overcoming the negative effects of preeclampsia [40,41,42]. These results indicate that pomegranate extract, either alone or in combination with standard therapy, has a significant effect in reducing kidney damage in preeclampsia, and has the potential to be used as an additional therapy to repair the kidney damage that occurs.
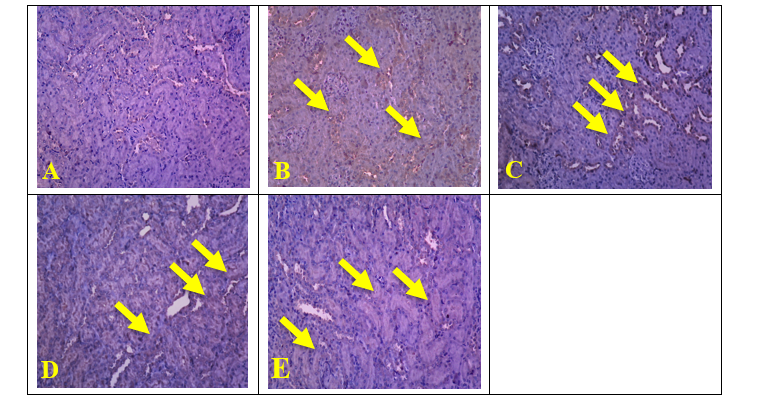
Figure 3 Effect of pomegranate extract on KIM-1 expression in the kidneys. KIM-1 expression was examined by immunohistochemical staining, showing positive expression in the cytoplasm of renal proximal tubule cells (yellow arrow). KIM-1 expression was negative in the normal pregnancy group (A) KIM-1 expression was higher in the preeclampsia group (B) KIM-1 expression was lower in the preeclampsia group treated with standard medication (C) and the preeclampsia group treated with pomegranate extract (D) The lowest KIM-1 expression was found in the preeclampsia group treated with standard medication combined with pomegranate extract (E) Immunohistochemical staining with anti-KIM-1 antibody at 200x magnification.
Effect of pomegranate extract on blood pressure
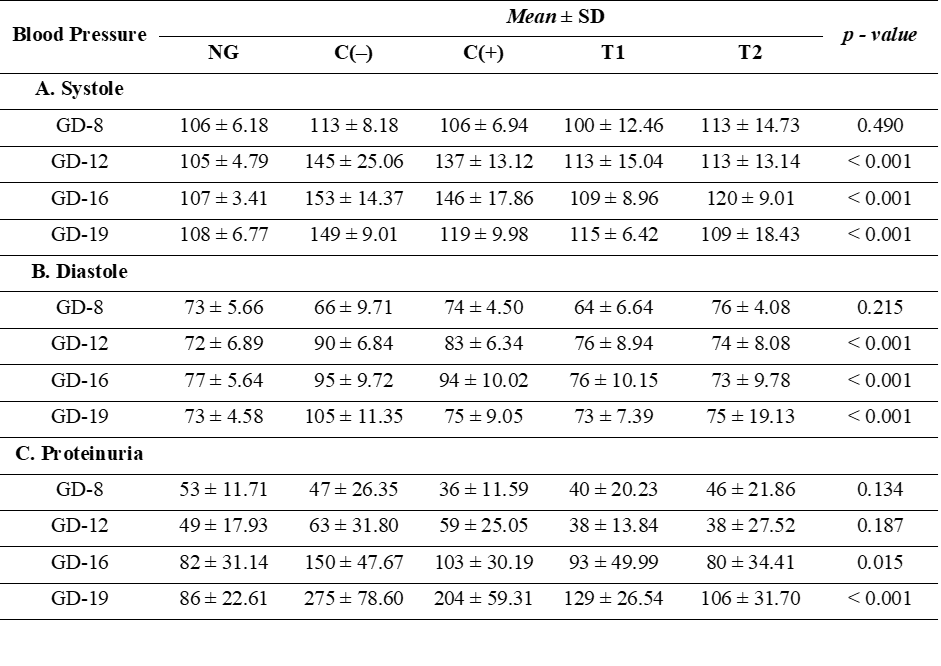
Pressure and proteinuria are key clinical indicators in the diagnosis of preeclampsia. Preeclampsia is characterized by a significant increase in blood pressure and the presence of protein in the urine (proteinuria), indicating impaired kidney function [43,44]. Repeated-measures ANOVA demonstrated significant effects of time (F = 21.120, p < 0.001), group (F = 19.82, p < 0.001), and time×group interaction (F = 5.670, p < 0.001) for systolic blood pressure. The untreated preeclampsia group showed the greatest increase over gestation, whereas the pomegranate-treated and combination groups showed attenuation of this progression. Repeated-measures ANOVA demonstrated significant effects of time (F = 13.732, p < 0.001), group (F = 13.86, p < 0.001), and time×group interaction (F = 6.163, p < 0.001) for diastolic blood pressure. The untreated preeclampsia group exhibited progressive elevation across gestation, whereas the treated groups showed a more controlled pattern. Therefore, these 2 parameters are highly relevant for assessing the effect of pomegranate extract in alleviating preeclampsia symptoms, particularly in the management of hypertension and kidney damage. Tables 2(A) and 2(B) shows that in the normal control NG group, systolic and diastolic blood pressure were at normal levels, reflecting good vascular function. In contrast, in the preeclampsia C(‒) group, blood pressure increased significantly due to impaired endothelial function and decreased NO production, leading to vasoconstriction and hypertension. Standard therapy C(+) showed a slight decrease in blood pressure, but still not reaching normal levels. The group given pomegranate extract T1 experienced a more significant decrease in blood pressure, indicating the extractʼs ability to increase NO production, improve vasodilation, and reduce vascular resistance. This decrease is consistent with previous research showing that pomegranate extract has an effective vasodilator effect in reducing hypertension in preeclampsia [14,44,45]. The combination of standard therapy and pomegranate extract T2 showed a greater synergistic effect in reducing systolic and diastolic blood pressure, indicating that pomegranate extract may enhance the effectiveness of antihypertensive therapy (Figures 4(A) and 4(B)).
Table 2 Differences in blood pressure (systolic and diastolic) and urine protein in preeclampsia rat models given pomegranate extract.
Description:
NG = Normal pregnant rats, C(‒) = Pregnant rats induced by L-NAME
75 mg/kgBW/day. C(+) = Pregnant rats induced by L-NAME treated with
standard MgSO4
(120 mg/kg), T1 = Pregnant rats induced by L-NAME treated with
pomegranate extract 500 mg/kgBW, T2 = Pregnant rats induced by
L-NAME treated with standard MgSO4
(120 mg/kg) and pomegranate extract 500 mg/kgBW/day.
Effect of pomegranate extract on proteinuria
Proteinuria in the untreated preeclampsia group increased progressively, reflecting ongoing renal injury. Repeated-measures ANOVA demonstrated significant effects of time (F = 104.650, p < 0.001), group (F = 11.62, p < 0.001), and time×group interaction (F = 9.254, p < 0.001) for proteinuria. The increase was attenuated in the pomegranate-treated and combination groups, supporting a renoprotective effect of the intervention. Progressive proteinuria reflects renal impairment; the moderated increase in treated groups aligns with reduced KIM-1 and improved vascular/endothelial markers. The group given standard therapy C(+) showed a decrease in proteinuria levels, but this was not significant compared to the PE group. The group given pomegranate extract T1 showed a significant decrease in proteinuria, indicating that pomegranate extract has the potential to protect the kidneys by reducing oxidative stress and inflammation. These findings support previous research showing that pomegranate extract can protect the kidneys from damage caused by oxidative stress [27,31]. The combination of pomegranate extract with standard therapy T2 showed a greater decrease in proteinuria, indicating a synergistic effect in improving kidney function and reducing further kidney damage (Figure 4(C)).
Renal protection was evidenced by the significant reduction in KIM-1 expression and attenuation of proteinuria progression. KIM-1 is a sensitive marker of tubular injury and reflects ongoing renal damage in hypertensive pregnancy models. The reduction of KIM-1 in treated groups suggests that pomegranate extract mitigates renal inflammatory and oxidative injury. These findings align with prior studies demonstrating the nephroprotective effects of polyphenol-rich plant extracts in experimental hypertension and inflammatory kidney injury.
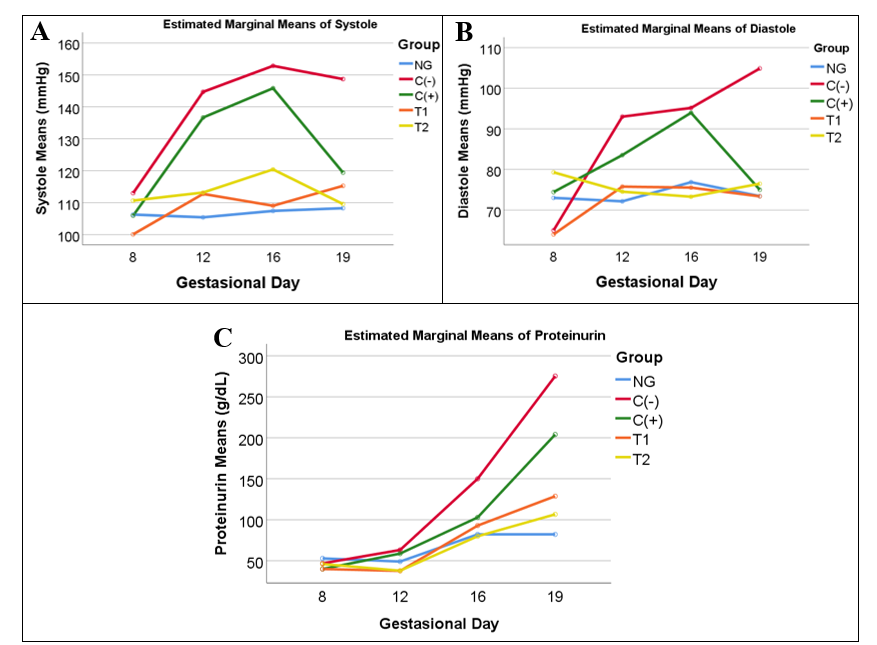
Figure 4 Longitudinal changes in clinical parameters of the experimental groups: (A) systolic blood pressure, (B) diastolic blood pressure, and (C) proteinuria, measured on gestational days 8, 12, 16, and 19.
Effect of Pomegranate Extract on Weight Fetus
Fetal weight is one of the important parameters in this study to assess the effect of pomegranate extract on fetal growth in the preeclampsia model. Table 1(F) shows that in the NG group, fetal weight was within the normal range (3.40 ± 0.33 g), indicating healthy fetal development without vascular disorders. In contrast, in the C(‒) group induced with L-NAME, fetal weight decreased to (3.20 ± 0.05 g), indicating a disturbance in placental blood flow and oxygen supply leading to Intrauterine Growth Restriction (IUGR). The C(+) group showed a decrease in fetal weight compared to the C(‒) group. This indicates that although antihypertensive therapy can lower blood pressure, it is not effective enough to restore vascular conditions and support optimal fetal growth. The (T1) group showed an increase in fetal weight to (3.41 ± 0.07 g), almost approaching the NG level. This improvement indicates that pomegranate extract, containing bioactive compounds such as flavonoids and ellagic acid, can repair vascular disorders in the placenta, increase blood flow, and improve oxygen and nutrient supply to the fetus. These results are consistent with research by Wang, which showed that pomegranate extract can increase blood flow to the placenta and support fetal development in pregnancy-related hypertension [19,46]. Meanwhile, in the group given combination therapy T2, the increase in fetal weight was more significant (3.47 ± 0.12 g) compared to the C(‒) and C(+) groups, indicating a synergistic effect of these 2 therapies. The combination of standard therapy and pomegranate extract provided greater improvements in increasing placental blood flow, restoring oxygen and nutrient balance, and supporting healthy fetal growth. The results of fetal weight measurements showed that pomegranate extract can improve fetal growth in preeclampsia. Administration of pomegranate extract, either alone or in combination with standard therapy, successfully increased fetal weight, indicating improved vascular conditions in the placenta and the restoration of optimal fetal growth. Combination therapy showed better results, improving pregnancy outcomes and supporting maternal and fetal health.
Conclusions
Pomegranate extract improved several key pathophysiological features of L-NAME–induced preeclampsia in rats. The intervention was associated with lower NF-κB levels, increased NO bioavailability, improved spiral artery diameter, reduced KIM-1 expression, moderated progression of blood pressure and proteinuria, and improved fetal weight. Although MDA levels showed a downward trend, the reduction was not statistically significant. These findings support the potential role of pomegranate extract as an adjunct therapeutic candidate in experimental preeclampsia.
Importantly, this study provides integrated experimental evidence that pomegranate extract exerts multi-target protective effects across vascular, renal, and fetal outcomes in a preeclampsia model, supporting its potential role as an adjunct therapy. Combination treatment with MgSO₄ showed enhanced protection on several endpoints, suggesting a synergistic benefit. Further studies are warranted to evaluate dose–response relationships, longer treatment windows, and underlying molecular mechanisms, as well as to support translation toward clinical investigation.
Acknowledgements
The authors wish to express their gratitude to the research supervisors from the Medical Sciences Study Program at the Faculty of Medicine, Universitas Sebelas Maret, and Universitas ‘Aisyiyah Surakarta. We also extend our sincere gratitude to the funders: Indonesian Education Scholarship (BPI), Center for Higher Education Funding and Assessment (PPAPT), and Indonesian Endowment Fund for Education (LPDP).
Declaration of Generative AI in Scientific Writing
In the process of preparing this manuscript, generative AI tools, specifically OpenAI’s ChatGPT, were employed to refine the language quality, rectify grammatical errors, and enhance text clarity, thereby improving the document's overall readability. Nevertheless, all scientific aspects of the study such as research design, methodology, data analysis, result interpretation, and the development of the discussion and conclusions were solely conceptualized and meticulously reviewed by the authors. The authors take full responsibility for the integrity, originality, and accuracy of both the research and the manuscript's content.
CRediT Author Statement
Endang Sri Wahyuni: Conceptualization, Research design, Methodology, Investigation, Formal analysis, Data curation, Writing – Original Draft. Soetrisno: Supervision, Conceptualization, Expertise in preeclampsia, Writing – Review and Editing. Bambang Purwanto: Supervision, Conceptualization, Validation, Writing – Review and Editing. Brian Wasita: Supervision, Methodology, Research design, Data analysis, Tissue examination preparation, Interpretation of results, Writing – Review and Editing. Vitri Widyaningsih: Data analysis, Research design, Methodology, Writing – Review & Editing. Risya Cilmiaty: Validation, Resources, Interpretation of result, Writing – Review and Editing. Paramasari Dirgahayu: Project administration, Methodology, supervision, Writing – Review & Editing.
References
[1] S Rana, E Lemoine, JP Granger and SA Karumanchi. Preeclampsia: Pathophysiology, challenges, and perspectives. Circulation Research 2019; 124(7), 1094-1112.
[2] P Guerby, A Swiader, N Augé, O Parant, C Vayssière, K Uchida, R Salvayre and A Negre-Salvayre. High glutathionylation of placental endothelial nitric oxide synthase in preeclampsia. Redox Biology 2019; 22, 101126.
[3] WD Pangesti, EPS Sasongko, A Pribadi and D Hilmanto. Evaluation of risk factor screening using the ministry of Health’s scoring system for the incidence of early-onset preeclampsia in primary health service. International Journal of Women’s Health 2025; 17, 4815-4822.
[4] V Dines, S Suvakov, A Kattah, J Vermunt, K Narang, M Jayachandran, CA Hassan, AM Norby and VD Garovic. Preeclampsia and the kidney: Pathophysiology and clinical implications. Comprehensive Physiology 2023; 13(1), 4231-4267.
[5] J Torres-Torres, S Espino-Y-Sosa, R Martinez-Portilla, H Borboa-Olivares, G Estrada-Gutierrez, S Acevedo-Gallegos, E Ruiz-Ramirez, M Velasco-Espin, P Cerda-Flores, A Ramirez-Gonzalez and L Rojas-Zepeda. A narrative review on the pathophysiology of preeclampsia. International Journal of Molecular Sciences 2024; 25(14), 7569.
[6] Y Wang, Y Jia, X Yang, B Liang, H Gao and T Yang. A potential role of Baicalin to inhibit apoptosis and protect against acute liver and kidney injury in rat preeclampsia model. Biomedicine and Pharmacotherapy 2018; 108, 1546-1552.
[7] R Aouache, L Biquard, D Vaiman and F Miralles. Oxidative stress in preeclampsia and placental diseases. International Journal of Molecular Sciences 2018; 19(5), 1496.
[8] D Ambarwati, F Fatmawati, M Nooryanto, S Santoso, SCW Baktiyani and N Nurdiana. Punica granatum fruit extract inhibits the production of pro-inflammatory cytokines and angiogenic factors of HUVEC cells induced by plasma from patients with pre-eclampsia. Clinical Nutrition Experimental 2017; 15, 9-14.
[9] W Yu, W Gao, D Rong, Z Wu and RA Khalil. Molecular determinants of microvascular dysfunction in hypertensive pregnancy and preeclampsia. Microcirculation 2019; 26(4), 12508.
[10] S Chaudhuri, B Banerjee, A Kumar and UK Biswas. Association between serum levels of nitric oxide and hydrogen sulfide in pre-eclampsia. Biochemistry & Analytical Biochemistry 2019; 8(3), 384.
[11] J Yuan, X Wang, Y Xie, Y Wang, L Dong, H Li and T Zhu. Circulating asymmetric dimethylarginine and the risk of preeclampsia: A meta-analysis based on 1338 participants. Oncotarget 2017; 8, 43944-43952.
[12] Andriyanti, Restiningsih, B Rahardjo, M Nooryanto, Sri Winarsih, N Permatasari and A Indriani. Effect of pravastatin on levels of malondealdehyde (MDA) and Endothelin-1 (ET-1) preeclampsia model rats. Malaysian Journal of Medicine and Health Sciences 2023; 19(1), 89-95.
[13] M Ożarowski, TM Karpiński, M Szulc, K Wielgus, R Kujawski, H Wolski and A Seremak-Mrozikiewicz. Plant phenolics and extracts in animal models of preeclampsia and clinical trials: Review of perspectives for novel therapies. Pharmaceuticals 2021; 14(3), 259.
[14] MY Ali, S Jannat and MS Chang. Discovery of potent angiotensin-converting enzyme inhibitors in pomegranate as a treatment for hypertension. Journal of Agricultural and Food Chemistry 2023; 71(30), 11476-11490.
[15] ES Wahyuni, L Firrahmawati, IN Mahmudah, JD Handayani and A Rahmawati. Potensi buah delima (Punica granatum) sebagai terapi adjuvan preeklampsia: A scoping review. Holistik Jurnal Kesehatan 2025; 19(5), 987-995.
[16] I Nasifah, S Soeharto and M Nooryanto. Effects of anti-lipid peroxidation of Punica granatum fruit extract in endothelial cells induced by plasma of severe pre-eclamptic patients. Journal of Ayurveda and Integrative Medicine 2017; 8, 215-217.
[17] LE Hosry, C Bou-Mitri, MB Dargham, MA Jaoudeh, A Farhat, JE Hayek, JMB Mosleh and E Bou-Maroun. Phytochemical composition, biological activities and antioxidant potential of pomegranate fruit, juice and molasses: A review. Food Bioscience 2023; 55, 103034.
[18] MI Kojadinovic, AC Arsic, JD Debeljak-Martacic, AI Konic-Ristic, ND Kardum, TB Popovic and MD Glibetic. Consumption of pomegranate juice decreases blood lipid peroxidation and levels of arachidonic acid in women with metabolic syndrome. Journal of the Science of Food and Agriculture 2017; 97(6), 1798-1804.
[19] Y Wang, M Huang, X Yang, Z Yang, L Li and J Mei. Supplementing punicalagin reduces oxidative stress markers and restores angiogenic balance in a rat model of pregnancy-induced hypertension. The Korean Journal of Physiology & Pharmacology 2018; 22(4), 409-417.
[20] D Wang, C Özen, IM Abu-Reidah, S Chigurupati, JK Patra, JO Horbanczuk, A Jóźwik, NT Tzvetkov, P Uhrin and AG Atanasov. Vasculoprotective effects of pomegranate (Punica granatum L.). Frontiers in Pharmacology 2018; 9, 00544.
[21] Y Zhao and F Zong. Inhibiting USP14 ameliorates inflammatory responses in trophoblast cells by suppressing MAPK/NF‐κB signaling. Immunity Inflammation and Disease 2021; 9(3), 1016-1024.
[22] BA Bakrania, EM George and JP Granger. Animal models of preeclampsia: Investigating pathophysiology and therapeutic targets. American Journal of Obstetrics Gynecology 2022; 226(2), 973-987.
[23] NWP Anggraini, S Sulistyowati, Soetrisno, B Purwanto and P Dirgahayu. Effect of moringa oleifera leaves on the expression of NFκβ, E-selectin, and superoxide dismutase in the placental of preeclamptic mouse model. Tropical Journal of Natural Product Research 2025; 9(4), 1800-1805.
[24] Y Anggraini, S Soetrisno, B Wasita and R Cilmiaty. Effects of olive leaf extract and nifedipine, alone and in combination, on blood pressure, neutrophil gelatinase-associated lipocalin, malondialdehyde, and creatinine levels in an Nω-nitro-L-arginine methyl ester-induced rat model of preeclampsia. Pharmacia 2024; 71, 122471.
[25] NZ Shaban, AA Sleem, MM Abu-Serie, AM Maher and NH Habashy. Regulation of the NF-κB signaling pathway and IL-13 in asthmatic rats by aerosol inhalation of the combined active constituents of Punica granatum juice and peel. Biomedicine & Pharmacotherapy 2022; 155, 113721.
[26] A Haseeb, NM Khan, OS Ashruf and TM Haqqi. A polyphenol‐rich pomegranate fruit extract suppresses NF‐κB and IL‐6 expression by blocking the activation of IKKβ and NIK in primary human chondrocytes. Phytotherapy Research 2017; 31(5), 778-782.
[27] JY Jang, D Kim, E Im and ND Kim. Therapeutic potential of pomegranate extract for women’s reproductive health and breast cancer. Life 2024; 14(10), 1264.
[28] N Maphetu, JO Unuofin, NP Masuku, C Olisah and SL Lebelo. Medicinal uses, pharmacological activities, phytochemistry, and the molecular mechanisms of Punica granatum L. (pomegranate) plant extracts: A review. Biomedicine and Pharmacotherapy 2022; 153, 113256.
[29] Z Yisimayili and Z Chao. A review on phytochemicals, metabolic profiles and pharmacokinetics studies of the different parts (juice, seeds, peel, flowers, leaves and bark) of pomegranate (Punica granatum L.). Food Chemistry 2022; 395, 133600.
[30] Z Yisimayili, R Abdulla, Q Tian, Y Wang, M Chen, Z Sun, Z Li, F Liu, HA Aisa and C Huang. A comprehensive study of pomegranate flowers polyphenols and metabolites in rat biological samples by high-performance liquid chromatography quadrupole time-of-flight mass spectrometry. Journal of Chromatography A 2019; 1604, 460472.
[31] K Matsubara, T Higaki, Y Matsubara and A Nawa. Nitric oxide and reactive oxygen species in the pathogenesis of preeclampsia. International Journal of Molecular Sciences 2015; 16(3), 4600-4614.
[32] J Kornacki, P Gutaj, A Kalantarova, R Sibiak, M Jankowski and E Wender-Ozegowska. Endothelial dysfunction in pregnancy complications. Biomedicines 2021; 9(12), 1756.
[33] M Moradnia, N Mohammadkhani, B Azizi, M Mohammadi, S Ebrahimpour, O Tabatabaei-Malazy, S Mirsadeghi and M Ale-Ebrahim. The power of punica granatum: A natural remedy for oxidative stress and inflammation; a narrative review. Journal of Ethnopharmacology 2024; 330, 118243.
[34] J Lo, CC Liu, YS Li, PY Lee, PL Liu, PC Wu, TC Lin, CS Chen, CC Chiu, YH Lai, YC Chang, HE Wu, YR Chen, YK Huang, SP Huang, SC Wang and CY Li. Punicalagin attenuates LPS-induced inflammation and ROS production in microglia by inhibiting the MAPK/NF-κB signaling pathway and NLRP3 inflammasome activation. Journal of Inflammation Research 2022; 15, 5347-5359.
[35] Fitriana, S Sulistyowati, D Indarto, S Soetrisno, I Nurwati and V Widyaningsih. Effect of kopyor coconut water on early-onset preeclampsia-like impairments in rats induced by L-nitro-arginine methyl ester. Pharmacia 2024; 71, 127575.
[36] MH Schoots, SJ Gordijn, SA Scherjon, HV Goor and JL Hillebrands. Oxidative stress in placental pathology. Placenta 2018; 69, 153-161.
[37] H Wang, M Li, P Chen and X Shi. Anti-inflammatory and antioxidant effects of pyrroloquinoline quinone in L-NAME-induced preeclampsia-like rat model. Reproductive Sciences 2022; 29, 578-585.
[38] HR Puneeth and SPS Chandra. A review on potential therapeutic properties of Pomegranate (Punica granatum L.). Plant Science Today 2020; 7(1), 9-16.
[39] Aditiawarman, MP Wardhana, LEP Sari and HT Joewono. The effect of l-arginine on diameter of spiral artery and fetal weight between normal pregnant mice and preeclampsia mouse models. International Journal of Pharmaceutical Research 2020; 12(4), 1413-1417.
[40] CX Shi, QH Qi, J Xu and WW Zhao. Protective effect of magnesium sulfate on cranial nerves in preeclampsia rats through the NF-κB/ICAM-1 pathway. European Review for Medical and Pharmacological Sciences 2020; 24(6), 2785-2794.
[41] W Sun, C Yan, B Frost, X Wang, C Hou, M Zeng, H Gao, Y Kang and J Liu. Pomegranate extract decreases oxidative stress and alleviates mitochondrial impairment by activating AMPK-Nrf2 in hypothalamic paraventricular nucleus of spontaneously hypertensive rats. Scientific Reports 2016; 6, 34246.
[42] A Radajewska, J Szyller, J Niewiadomska, A Noszczyk-Nowak and I Bil-Lula. Punica granatum L. polyphenolic extract as an antioxidant to prevent kidney injury in metabolic syndrome rats. Oxidative Medicine and Cellular Longevity 2023; 2023, 6144967.
[43] F Fitriana, Soetrisno, S Sulistyowati and D Indarto. Evaluation of placental bed uterine in L-NAME-induced early-onset preeclampsia (EO-PE) like the rat model. Turkish Journal of Obstetrics and Gynecology 2024; 21(3), 180-189.
[44] Z Pánczél, Z Kukor, D Supák, B Kovács, A Kecskeméti, R Czizel, M Djurecz, B Alasztics, KB Csomó, A Hrabák and S Valent. Pravastatin induces NO synthesis by enhancing microsomal arginine uptake in healthy and preeclamptic placentas. BMC Pregnancy Childbirth 2019; 19, 426.
[45] ES Wahyuni, Soetrisno, B Purwanto, B Wasita, V Widyaningsih, R Cilmiaty and P Dirgahayu. Pomegranate extract as a natural therapy for preeclampsia: Enhancing endothelial function, modulating inflammation, and boosting antioxidant activity. Trends in Sciences 2026; 23(5), 12241.
[46] SL Finn-Sell, EC Cottrell, SL Greenwood, MR Dilworth, EJ Cowley, CP Sibley and M Wareing. Pomegranate juice supplementation alters utero-placental vascular function and fetal growth in the eNOS-/- mouse model of fetal growth restriction. Frontiers in Physiology 2018; 9, 1145.