Trends
Sci.
2026;
23(8):
13036
Neurobiological and Clinical Effects of Vitamin D in Psychiatric Symptoms:
A Meta-Analysis and Systematic Review
Rina Hastuti Lubis1, Hanifah Yusuf2,*, Khairan Khairan3 and Nirwana Lazuardi Sary4
1Doctoral Program of Medical Science, Faculty of Medicine, Universitas Syiah Kuala, Aceh 23111, Indonesia
2Department of Pharmacology, Faculty of Medicine, Banda Aceh, Universitas Syiah Kuala, Aceh 23111, Indonesia
3Department of Pharmacy, Faculty of Mathematics and Natural Sciences, Universitas Syiah Kuala,
Aceh 23111, Indonesia
4Departement of Physiology, Faculty of Medicine, Universitas Syiah Kuala, Aceh 23111, Indonesia
(*Corresponding author’s e-mail: [email protected])
Received: 15 December 2025, Revised: 27 December 2025, Accepted: 10 January 2026, Published: 20 March 2026
Abstract
Beyond its traditional function in maintaining calcium and phosphate homeostasis, vitamin D is now widely understood as a neuroactive steroid with regulatory effects on neural transmission, inflammatory modulation, and synaptic adaptability commonly referred to as neuroplasticity. Insufficient vitamin D status has been linked to disturbances in neuroimmune regulation as well as dysregulation of key neurotransmitter systems including dopaminergic, serotonergic, and glutamatergic pathways. This meta-analysis integrates findings from neurobiological research and clinical trials to examine the impact of vitamin D supplementation on a range of psychiatric manifestations, encompassing depressive symptoms, anxiety, psychotic features, and substance-related psychiatric disturbances. A total of 16 randomized controlled trials published between 2016 and 2025 were included, with data synthesized using a random-effects model and standardized assessment instruments such as the BDI, HAM-D, PHQ-9, BAI, STAI-S, and PANSS. The aggregated results indicate that vitamin D supplementation is associated with a small to moderate reduction in overall psychiatric symptom severity, as reflected by a standardized mean difference of −0.33 with a 95% confidence interval ranging from −0.54 to −0.12 and a statistically significant p value of 0.002. More consistent improvements were observed in mild-to-moderate depressive symptoms (SMD = −0.40; 95% CI −0.68 to −0.13; p = 0.004). Among individuals with substance use disorders, vitamin D significantly lowered depressive symptom scores (MD = −3.60; 95% CI −5.19 to −2.00; p < 0.0001), whereas its effects on anxiety symptoms were not significant (SMD = −0.74; 95% CI −1.71 to 0.23; p = 0.14). In psychotic disorders, vitamin D produced no significant improvements across PANSS domains (p > 0.05). vitamin D appears to modulate excitatory-inhibitory neurotransmission, oxidative stress regulation, inflammatory signaling, and monoaminergic pathways, supporting its role as an adjuvant rather than a primary therapeutic agent. Although beneficial in specific clinical contexts, vitamin D shows limited efficacy in severe psychiatric conditions characterized by longstanding neurocircuit abnormalities. Future large-scale RCTs are needed to determine optimal dosing strategies and clinical subgroups most likely to benefit.
Keywords: Vitamin D, Psychiatric symptoms, Depression and anxiety, Psychosis, Randomized controlled trials
Introduction
In addition to its established endocrine functions, vitamin D plays an important role in central nervous system physiology by influencing synaptic activity, inflammatory responses, and neural plasticity. Accumulating evidence suggests that insufficient vitamin D status is linked to disturbances in neuroimmune regulation as well as alterations in dopaminergic, serotonergic, and glutamatergic signaling, all of which are central to the pathophysiology of psychiatric disorders [1-3].
Globally, the burden of psychiatric disorders has continued to rise over the past 3 years. The most recent WHO report estimates that more than one billion individuals are currently living with mental health conditions, indicating a substantial increase in global psychiatric service needs [4]. These data are consistent with findings from the Global Burden of Disease (GBD), which reported that approximately 970 million people were affected by mental disorders in 2019, encompassing depression, anxiety, schizophrenia, and substance use disorders [5]. Depression also remains the leading global cause of years lived with disability (YLD), particularly among working-age adults [6]. These epidemiological trends underscore the urgency of identifying biological factors and potential therapeutic interventions that may improve prevention and management strategies for psychiatric disorders.
During the COVID-19 pandemic and post-pandemic periods, global modelling based on GBD 2019 estimates demonstrated substantial increases in major depressive disorder (an additional 53.2 million cases, +27.6%) and anxiety disorders (an additional 76.2 million cases, +25.6%), with disproportionately greater impacts in low- and middle-income countries [7]. More recent international assessments estimate that approximately 301 million people currently live with anxiety disorders and around 280 million with depression, reflecting more than a 50% increase since 1990 and a sustained upward trajectory over the last decade [5,8]. Among populations with substance use disorders, systematic reviews have shown markedly elevated psychiatric comorbidity: individuals with common mental disorders are approximately twice as likely to develop alcohol use disorder, while those with alcohol use disorder have a 3.1-fold higher risk of experiencing depressive symptoms [9,10] Psychotic disorders, including schizophrenia, also remain major contributors to global disease burden, with incidence estimates ranging from 15 to 30 cases per 100,000 individuals per year [11].
Although numerous observational studies have reported associations between low serum 25-hydroxyvitamin D levels and increased risk of depression, anxiety, or psychotic symptoms, interventional evidence from randomized controlled trials (RCTs) remains heterogeneous. Several recent meta-analyses have suggested that vitamin D supplementation may reduce depressive symptom scores over short-term follow-up in adults [12,13]. However, other trials have not demonstrated significant benefits among individuals with psychotic disorders or substance-related psychiatric symptoms [14]. These inconsistencies raise important questions regarding whether vitamin D exerts meaningful effects on anxiety, psychotic symptoms, or neurocognitive functioning, while the underlying neurobiological mechanisms remain incompletely defined [15]. Variability in dosing regimens, treatment duration, baseline vitamin D status, and clinical or demographic characteristics across trials further contributes to this heterogeneity.
Despite growing research interest, the magnitude and consistency of vitamin D’s neurobiological and clinical effects across different psychiatric symptom domains remain unclear, including primary depression, primary anxiety, primary psychotic symptoms, and substance-related depressive or anxiety symptoms. Most existing systematic reviews have examined isolated diagnostic categories and have rarely integrated mechanistic neurobiological evidence with clinical outcome data. Consequently, an important research gap remains regarding a comprehensive synthesis of both neurobiological mechanisms and clinical effects of vitamin D across diverse psychiatric domains. Addressing this gap offers theoretical relevance by clarifying vitamin D’s role in modulating neurotransmission and neuroinflammation across diagnostic boundaries, as well as practical implications for evaluating its potential use as an adjunctive therapeutic strategy. This meta-analysis aims to address this gap by synthesizing recent randomized controlled trials evaluating vitamin D supplementation and psychiatric outcomes.
Materials and methods
The methodology in this research was structured as follows:
Research design
A random-effects model was applied in this meta-analysis to appropriately account for variation across studies. Although all included trials were randomized controlled designs, the studies naturally differed in several methodological and clinical aspects. This variability reflected differences in participant characteristics such as age range, baseline vitamin D status, psychiatric diagnoses, and comorbid medical conditions,as well as prior treatment exposure and initial symptom severity. The vitamin D intervention regimens also varied in terms of dosage, frequency, route of administration, and study duration, which is expected in multi-center and multi-population clinical research. Differences were likewise present in outcome assessment procedures, including the use of various validated psychiatric rating scales and their measurement schedules. Additionally, the studies were conducted across diverse healthcare and community settings, contributing to the expected breadth of clinical contexts. These forms of methodological diversity are common in meta-analyses of clinical trials and were carefully accounted for when interpreting the pooled estimates [16].
Setting and samples
This meta-analysis covered research published over the past ten years (2016 - 2025), drawing evidence from major electronic databases, including PubMed, the Cochrane Library, and Scopus. Studies were identified and selected through a sampling framework based on predefined eligibility criteria. The inclusion criteria comprised: (1) randomized controlled trials (RCTs) investigating the impact of Vitamin D supplementation on psychiatric symptoms; (2) studies employing validated psychiatric assessment instruments appropriate for each diagnostic subgroup,psychotic, depressive, and anxiety disorders, such as PANSS, BDI, HAM-D, CES-D, HADS-D, PHQ-9, BAI, STAI-S, and HADS-A; and (3) trials reporting quantitative outcomes in the form of mean ± standard deviation (SD). Studies lacking a control group or failing to report outcomes as mean ± SD were excluded. Following application of these criteria, 16 RCTs were deemed eligible, encompassing 9,947 participants in the intervention groups and 9,752 in the control groups. The final sample size reflected the total number of studies meeting all inclusion requirements.
Intervention
This meta-analysis integrates findings from randomized controlled trials that examined how Vitamin D influences both neurobiological processes and clinical outcomes across diverse psychiatric conditions. The trials included in this review utilized a wide range of supplementation approaches, reflecting differences in Vitamin D formulations, dosing regimens, and treatment durations. Each study featured an appropriate comparison group,either placebo or standard care, selected in accordance with its methodological design and the specific psychiatric population under investigation.
Measurement and data collection
Data collection involved extracting relevant information from each included study using a standardized data extraction form. The extracted variables included study characteristics (author, year, and country), participant demographics (sample size and age range), baseline clinical status, study design, duration, and details of the Vitamin D intervention (formulation, dosage, administration route, and frequency), along with the corresponding control conditions. The primary outcomes were changes in psychiatric symptoms, assessed using validated instruments such as the BDI, BAI, PHQ-9, CES-D, HADS, STAI-S, MADRS, HAM-D 17, HDRS-17, and PANSS (Total, Positive, Negative, General). The reliability of these scales is well established, and data extraction was performed independently to ensure accuracy, with any discrepancies resolved through consensus.
Data analysis
Statistical processing was conducted using Review Manager (RevMan) software version 5.4. Effect estimates for continuous variables were expressed as standardized mean differences or mean differences accompanied by 95% confidence intervals. A random-effects analytical approach was employed to accommodate potential clinical and methodological diversity among the included studies. The extent of heterogeneity was evaluated through the I² statistic, with threshold values of 25% indicating low heterogeneity, 50% representing moderate heterogeneity, and 75% reflecting a high degree of heterogeneity [17]. Subgroup analyses were performed based on diagnostic categories, including primary depressive disorder, depressive or anxiety symptoms related to substance use, primary anxiety symptoms, and psychotic disorders (PANSS subdomains). The subgroup analyses revealed differing degrees of heterogeneity that aligned with variations in population profiles, initial vitamin D status, supplementation dosage protocols, and the psychiatric assessment instruments applied. Potential publication bias was examined through visual appraisal of funnel plot symmetry, while sensitivity analyses were performed by sequentially removing individual studies to determine the stability and reliability of the pooled effect estimates.
Trustworthiness/rigor
This section does not apply to the present investigation because the study was designed as a quantitative meta-analysis rather than a qualitative exploration. Even so, the methodological rigor of the included randomized trials was systematically evaluated using the Cochrane Risk of Bias Tool. This instrument assesses potential bias across several critical domains, encompassing the generation of random sequences, concealment of allocation procedures, blinding of participants and research personnel, blinding of outcome assessors, completeness of outcome data, and the presence of selective outcome reporting [18,19]. Each study was rated as having a low, high, or unclear risk of bias. Two reviewers (author 1 and author 2) independently conducted the assessments, with disagreements resolved through consultation with a third reviewer (author 3).
Ethical considerations
This meta-analysis relied exclusively on data extracted from previously published research and therefore did not entail any direct involvement of human or animal participants. Consequently, ethical approval and informed consent were not required for the present work. All primary studies included in the review were presumed to have obtained the necessary ethical clearances, as documented within their respective publications.
Results and discussion
Included studies
The modified PRISMA flow diagram shown in Figure 1 summarizes the process of study identification and selection undertaken in this systematic review. An initial search of the Scopus, Cochrane Library, and PubMed databases yielded 657 records. After the removal of 20 duplicate entries, 637 records remained for screening. Title and publication type screening resulted in the exclusion of 610 records that did not meet the relevance criteria. A total of 27 full-text articles were subsequently identified for retrieval, of which 24 were successfully accessed. After assessment for eligibility, 8 articles were excluded, comprising 4 studies that did not report baseline measurements prior to intervention and 4 publications classified as review papers, short communications, editorials, or news articles.
Ultimately, 16 randomized controlled trials (RCTs) were included in the final review. Across these 16 RCTs [14,20-34], a total of 9,947 participants were allocated to the intervention groups and 9,752 to the control groups. The characteristics of the included studies are summarized in Table 1. Data extraction was conducted using a customized form that captured study demographics, clinical characteristics, diagnostic criteria, trial design, vitamin D supplementation regimen, dosage, duration of therapy, comparator conditions, and the psychiatric rating scales employed across studies. All extracted data were independently verified by a third reviewer, and authors were contacted when clarification regarding unclear or missing data was required.
Quality assessment
The assessment of bias related to efficacy outcomes for each randomized controlled trial is presented in Figure 2(A), whereas Figure 2(B) summarizes the overall risk of bias across the entire set of included trials. The findings indicate that the greatest contribution to aggregate bias arises from ancillary factors. Based on the quality appraisal, all studies incorporated in the analysis employed randomized controlled trial designs, and the individual risk of bias for each trial was evaluated as low.
Efficacy of vitamin D
Based on Figures 3(A) - 3(E), this meta-analysis indicates that vitamin D supplementation offers meaningful benefits for mental health, particularly in reducing general psychiatric symptoms. Drawing on data from 16 studies involving 19,699 participants, vitamin D was associated with a small-to-moderate improvement in overall psychiatric symptom severity (SMD = −0.33, 95% CI −0.54 to −0.12; p = 0.002), although substantial heterogeneity was observed across trials. In populations with substance use disorders, vitamin D supplementation led to a clear and significant reduction in depressive symptoms (MD = −3.60, 95% CI −5.19 to −2.00; p < 0.0001), yet its impact on anxiety symptoms within this group was inconsistent. Among individuals in psychotic disorders, vitamin D did not demonstrate significant effects on positive.
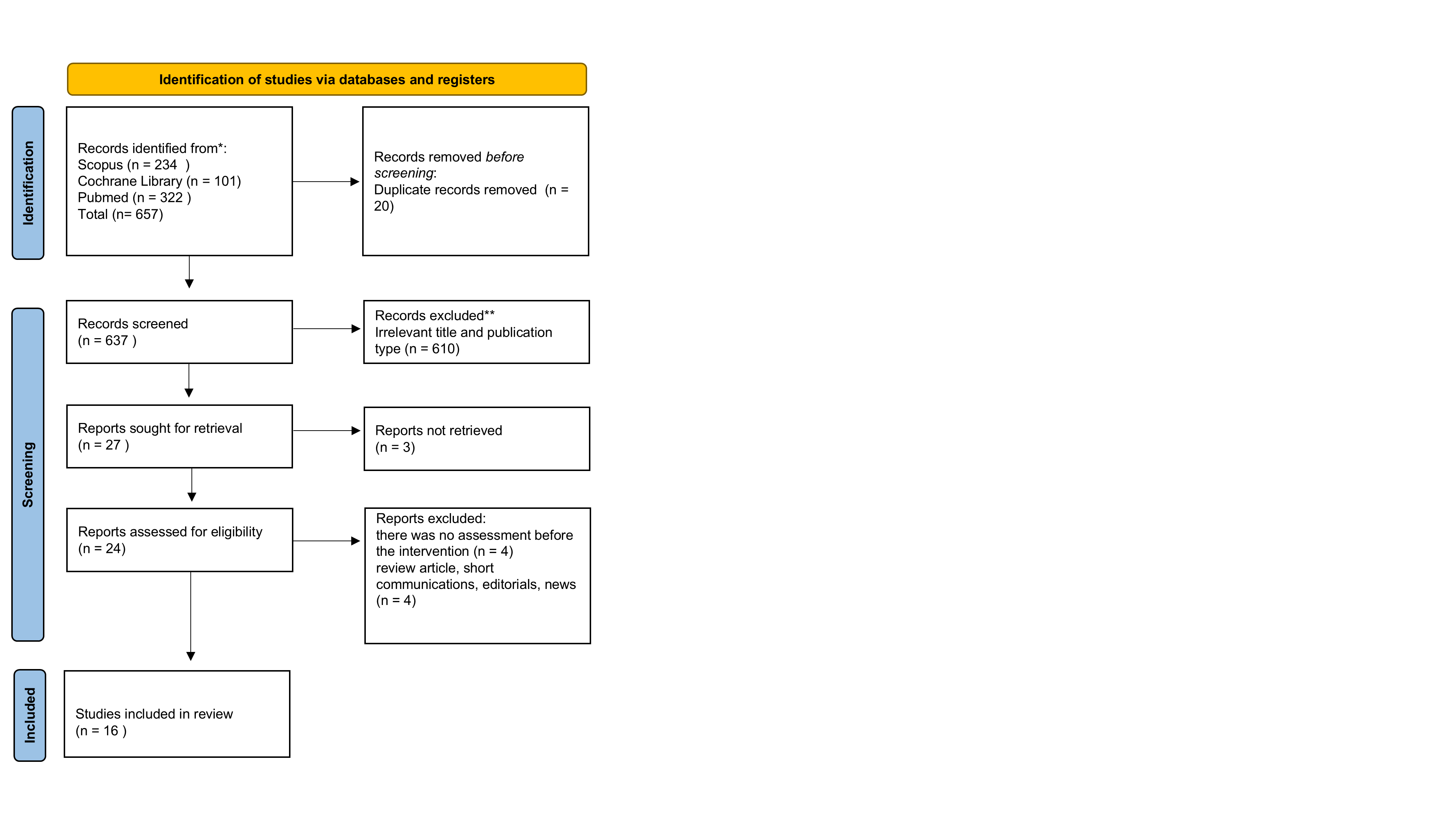
Figure 1 PRISMA flow diagram showing the process of study identification, screening, eligibility assessment, and inclusion of randomized controlled trials (RCTs) in the meta-analysis.
Table 1 Characteristics of RCTs included for meta-analysis.
Author / Country |
Population and Total Sample |
Diagnosis / Baseline Characteristics |
Study Design & Duration |
Vitamin D Intervention |
Control Condition |
Psychiatric Scale Used |
Choukri et al. [20] - New Zealand |
152 healthy women, (age 18 - 40 years) |
Healthy premenopausal women; baseline vitamin D varied; no clinical depression |
Double-blind RCT; 6 months |
50,000 IU vitamin D₃ monthly |
Placebo (identical capsule) |
CES-D and HADS-Anxiety Subscale |
Karami-Mahajeri et al. [21] - Iran |
60 Healthy students (age 20 - 25 years) |
University students without medical illness; baseline 25(OH)D measur ed |
Double-blind RCT; 8 weeks |
Two pearls of 50,000 IU vitamin D₃, given at baseline and week 4 |
Placebo softgel |
HADS-Anxiety and HADS-Depression |
Zaromytidou et al. [22] - Greece |
90 Elderly patients with prediabetes (age > 60 years) |
Elderly adults with prediabetes; baseline vitamin D deficiency in > 90% |
Open-label RCT; 12 months |
Vitamin D₃ 25,000 IU weekly |
No supplementation (lifestyle advice only) |
STAI-S (Anxiety) and PHQ-9 (Depression) |
Ghaderi et al. [23] - Iran |
68 Methadone Maintenance Treatment (MMT) patients (age 25 -70 years) |
Opioid Use Disorder on MMT |
double-blind RCT; 12 weeks |
Vitamin D₃ 50,000 IU every 2 weeks |
Placebo |
BDI and BAI |
Ghaderi et al. [14] - Iran |
64 MMT patients (age 18 - 60 years) |
Opioid Use Disorder on MMT |
double-blind RCT; 24 weeks |
Vitamin D₃ 50,000 IU every 2 weeks |
Placebo |
BDI and BAI |
Gaughran et al. [24] (DFEND Trial), UK |
149 participants First‐episode psychosis (FEP) (age 18 - 65 years) |
FEP within 3 years of first presentation; high Vit D deficiency |
Multisite, double-blind, RCT; 6 months; |
120,000 IU monthly for 6 months; Oral liquid (6 mL per dose). |
Placebo oil (organoleptically identical) administered monthly. |
PANSS (Total, Positive, Negative, General |
Krivoy et al. [25] - Israel |
47 patients Chronic schizophrenia (age 22 - 65) |
Chronic schizophrenia treated with clozapine ≥ 18 weeks; DSM-IV-TR diagnosis confirmed by 2 psychiatrists; Baseline vitamin D < 75 nmol/L; PANSS total > 70; Age 18 - 65 yrs. |
Double-blind, RCT; Duration 8 weeks |
Vitamin D3 14,000 IU weekly (35 drops; 0.35 mg) supervised dosing, 8 weeks. |
Matching placebo oral drops, same schedule. |
PANSS (Total, Positive, Negative, General) |
Sheikhmoonesi et al. [26] - Iran |
80 male patients with chronic stable schizophrenia (18 - 65 years) |
schizophrenia; illness > 3 years; residual symptoms; all on stable antipsychotic dose ≥ 2 months; baseline Vit D < 30 ng/mL; BMI 16 - 25 kg/m² |
Open-label, parallel-group RCT; 3 months follow-up |
Two intramuscular injections of Vitamin D₃ (300,000 IU/mL, total 600,000 IU) at baseline + standard antipsychotic regimen |
Standard antipsychotic regimen only |
PANSS (Positive and Negative Syndrome Scale) |
Vellekkatt et al. [27] - India |
46 adults with MDD (age 18 - 65 years) |
Major depressive disorder; Vit D deficiency < 20 ng/mL; antidepressant-naive |
Double-blind RCT; 12 weeks |
300,000 IU cholecalciferol IM (single dose) |
Placebo (normal saline) |
HDRS-17 |
Hansen et al. [28] Denmark |
62 adults with depression (age 18 - 65 years) |
ICD-10 depressive episode (F32.x), mild-severe |
Double-blind RCT; 6 months |
70 μg (2800 IU) Vitamin D3 daily |
Placebo |
HAM-D 17 |
Libuda et al. [29] - Germany |
113 children & adolescents (age 11 - 18 years) |
BDI-II > 13; Vitamin D ≤ 30 nmol/L |
Double-blind RCT; 28 days |
2640 IU Vitamin D3 daily |
Placebo |
BDI-II |
Kaviani et al. [30] - Iran |
56 adults (age 18 - 60 years) |
Mild-moderate depression; BDI-II 14-28 |
Double-blind RCT; 8 weeks |
50,000 IU Vitamin D every 2 weeks |
Placebo |
BDI-II |
Kumar et al. [31] - India |
59 adults with MDD (age 18 - 60 years) |
HAM-D ≥ 15; Vit D < 20 ng/mL |
Double-blind RCT; 12 weeks |
60,000 IU Vitamin D every 5 days + escitalopram |
Placebo + escitalopram |
HAM-D 17; MADRS; BDI |
Satyanarayana et al. [32] - India |
451 adolescents (age 10 - 19 years) |
Depressive symptoms based on BDI-II |
Cluster RCT; 9 weeks |
2250 IU Vitamin D daily |
250 IU/day (low-dose Vit D) |
BDI-II |
Putranto et al. [33] - Indonesia |
70 adults with T2DM + depression (age 30 - 65 years) |
Mild-moderate depression (BDI-II); Vit D deficiency |
Double-blind RCT; 12 weeks |
4000 IU cholecalciferol daily |
Placebo |
BDI-II |
Rahman et al. [34] - Australia |
21,315 older adults (age 60 - 84 years) |
General population; PHQ-9 depressive symptoms |
Double-blind RCT; 5 years |
60,000 IU Vitamin D3 monthly |
Placebo |
PHQ-9 |

Figure 2 (A) The first figure shows the risk-of-bias assessment for each RCT across 7 domains, rated as low (green), unclear (yellow), or high (red). (B) The second figure presents a bar chart summarizing the distribution of these ratings across all included trials. Overall, the figures demonstrate that the studies generally exhibit a low risk of bias, with only minor variability observed in a few domains.
Negative, general, or total PANSS scores, suggesting limited clinical benefit as an adjunctive treatment in schizophrenia. A nuanced pattern also emerged in studies examining depressive outcomes: while vitamin D effectively reduced depressive symptoms in community samples and individuals with mild-to-moderate symptom levels (SMD = −0.40, 95% CI −0.68 to −0.13; p = 0.004), it did not yield significant improvements in patients with clinically diagnosed depressive disorder (SMD = −0.26, 95% CI −0.75 to 0.23; p = 0.30).
Similarly, the overall effect of vitamin D on anxiety symptoms was not statistically significant (SMD = −0.74, 95% CI −1.71 to 0.23; p = 0.14), with considerable variability across studies. The pooled anxiety outcome was non-significant and characterized by substantial heterogeneity, reflecting uncertainty in the current evidence base. Differences in study design, baseline symptom severity, and intervention characteristics may have contributed to this heterogeneity.
Taken together, these findings suggest that vitamin D may hold the greatest therapeutic value for individuals experiencing mild-to-moderate psychiatric symptoms, particularly depressive symptoms, while offering more limited benefit in severe conditions such as schizophrenia, depressive disorder, and generalized anxiety. The wide variability across studies likely reflects differences in baseline vitamin D status, dosage, treatment duration, and population characteristics.
From a clinical perspective, these findings support the potential relevance of assessing vitamin D status in individuals presenting with mild-to-moderate depressive symptoms, particularly given the low cost and favorable safety profile of supplementation. From a research standpoint, the observed heterogeneity underscores the need for future biomarker-based and dose-response randomized controlled trials. These results highlight the need for future large-scale, rigorously designed trials to clarify the specific clinical contexts in which vitamin D supplementation may be most effective and to deepen our understanding of its potential role in mental health care.
Publication bias
Funnel plot analysis demonstrated generally symmetrical distributions across all symptom domains, indicating minimal publication bias [35,36]. Figure 3(A), which summarizes overall psychiatric symptoms, shows a balanced spread of effect sizes around the pooled estimate, suggesting low heterogeneity and negligible publication bias. Figure 3(B) shows depressive symptom outcomes with an overall symmetrical distribution, indicating minimal publication bias, although the wider spread of data points suggests greater inter-study variability. Panel C, representing psychotic symptoms (PANSS outcomes), also shows a stable distribution with minimal deviation from the central effect, reflecting the absence of visible publication bias. Figure 3(D) illustrates anxiety symptom outcomes, demonstrating a similarly symmetrical pattern.
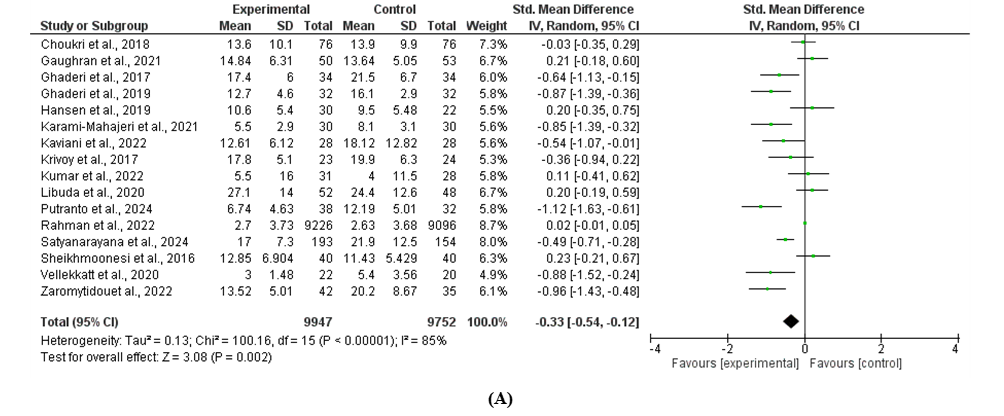
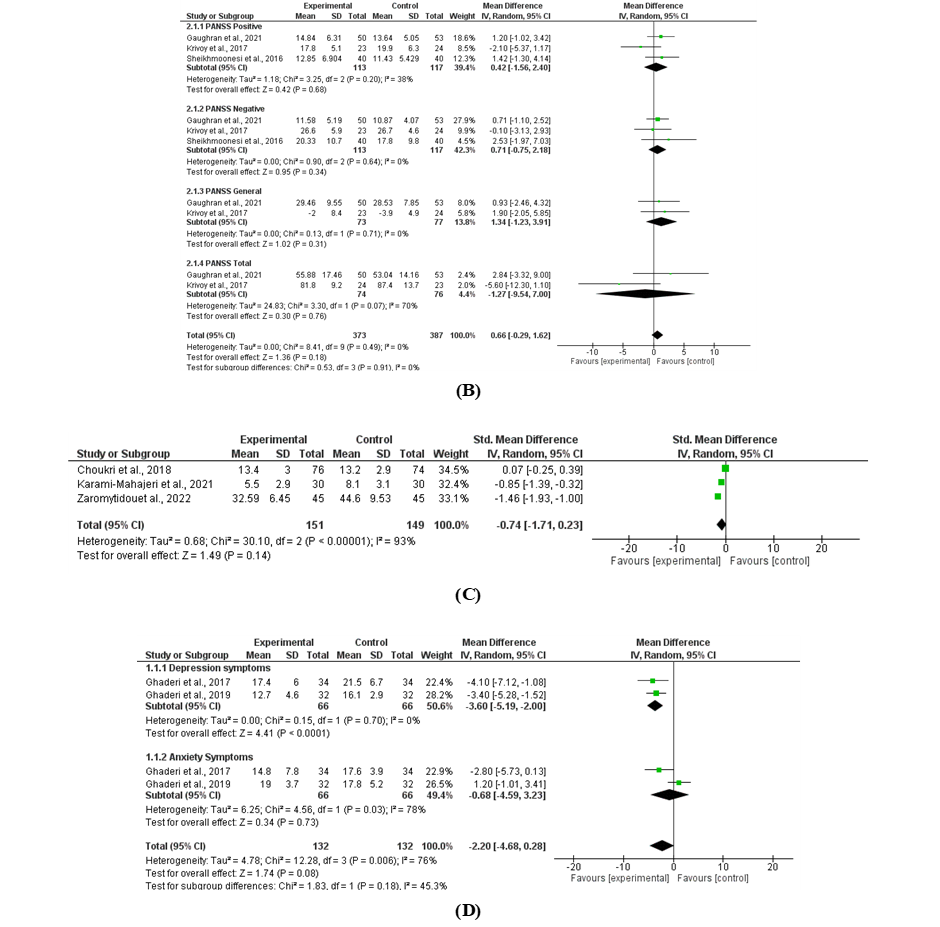
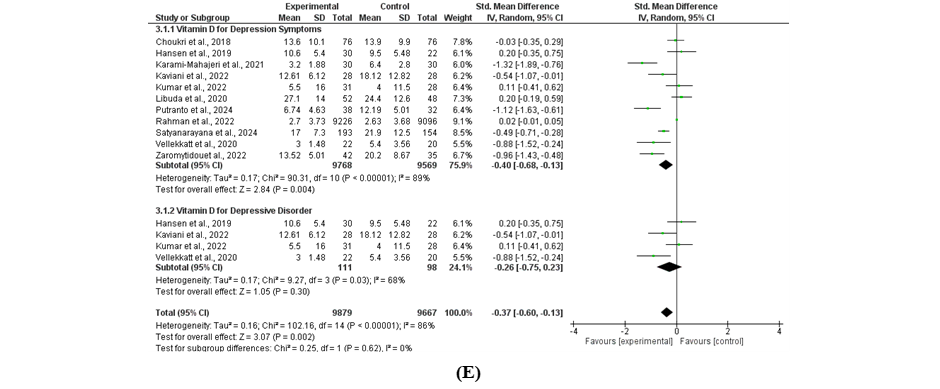
Figure 3 Forest plots of the effects of vitamin D supplementation on psychiatric outcomes (A) psychiatric symptoms, (B) psychotic disorder, (C) anxiety symptoms, (D) depressive and anxiety symptoms in substance use disorders and (E) depressive symptoms and depressive disorder.
Finally, Figure 4(A) which displays substance-use-related psychiatric symptoms, shows an overall symmetrical funnel shape, supporting minimal publication bias across included studies. Taken together, the symmetrical patterns across Figures 4(A) - 4(E) support the robustness of the pooled estimates and indicate that the results are unlikely to be affected by systematic publication bias.
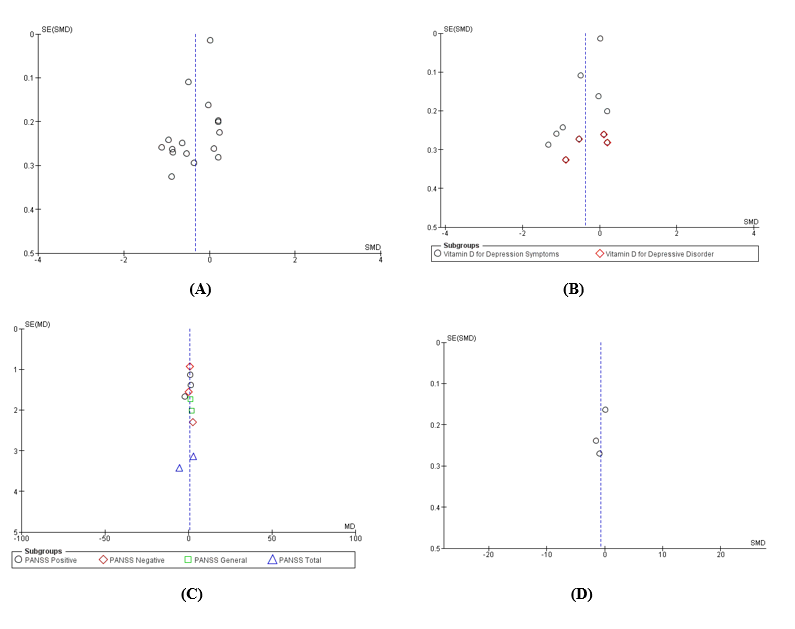
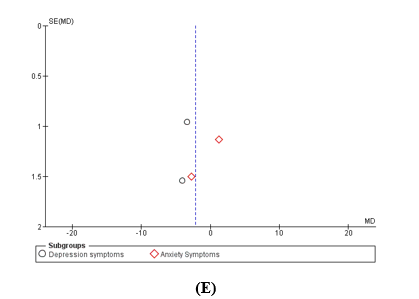
Figure 4 Funnel plot analyses demonstrated generally symmetrical distributions across all symptom domains, indicating low heterogeneity and minimal publication bias; (A) the distribution for overall psychiatric symptoms, (B) depressive outcomes, showing good symmetry across studies, (C) psychotic symptoms (PANSS domains), with minimal dispersion and no visible publication bias, (D) anxiety outcomes, showing a stable and symmetrical pattern and (E) substance-use-related psychiatric symptoms, also demonstrating overall symmetry.
From a neurobiological standpoint, vitamin D has come to be regarded as a neuroactive steroid with effects mediated by the vitamin D receptor (VDR), which is widely expressed in cortical and limbic structures that play central roles in mood regulation, emotional integration, and cognitive function [3,37,38]. Activation of the vitamin D receptor facilitates modulation of gene expression linked to neurotrophic signaling, regulation of ion channel function, and preservation of long-term synaptic integrity. Taken together, these genomic actions support adaptive forms of neuroplasticity and enhance neuronal resistance to a range of neurobiological stressors [3,37-39].
In addition, vitamin D exerts rapid non-genomic effects on neurons and glial cells, including modulation of intracellular calcium homeostasis, regulation of glutamate and GABA signaling, and attenuation of excitotoxicity, mechanisms that are highly relevant to the pathophysiology of depression, anxiety, and psychosis [3,37,38].
The non-genomic effects of vitamin D are mediated through membrane-associated receptors such as PDIA3 and extranuclear VDR. At the membrane level, interactions between 1,25-dihydroxyvitamin D and PDIA3 initiate intracellular signaling cascades that rapidly influence calcium dynamics and downstream kinase activity, which subsequently increases the production of inositol-1,4,5-triphosphate (IP₃) and triggers the rapid release of Ca²⁺ from the endoplasmic reticulum, followed by activation of downstream kinase cascades including PKC, PI3K, and MAPK/ERK. These mechanisms have been comprehensively described in reviews on nongenomic vitamin D signaling and studies of vitamin D₃-induced neuroprotection, which highlight the central role of PDIA3 as a key mediator of non-genomic responses and a regulator of intracellular Ca²⁺ homeostasis [40-42]. The rapid alterations in intracellular Ca²⁺ subsequently influence neuronal excitability, synaptic transmission, and neuronal survival. Reviews on vitamin D and the central nervous system further demonstrate that, within brain tissue, vitamin D contributes to stabilizing Ca²⁺ homeostasis and protects neurons from calcium overload, a process known to precipitate excitotoxicity and synaptic injury associated with depression, anxiety, and psychosis [43-45].
At the neurotransmitter level, vitamin D modulates the glutamate-GABA system. Experimental studies in animal and cellular models have shown that vitamin D deficiency reduces the expression of glutamate decarboxylase 65/67 (GAD65/67), the key enzymes responsible for GABA synthesis, and disrupts the balance between glutamate and GABA, whereas vitamin D supplementation restores the expression of these enzymes and normalizes the associated pathways. This is supported by molecular regulatory studies of the CNS and by reviews on synaptic function and vitamin D-related circuitry in neurodevelopmental disorders, both of which report alterations in GAD65/67 and other neurotransmitter-related enzymes as consequences of vitamin D status [46,47].
In addition, Vitamin D supports cellular redox balance by strengthening endogenous antioxidant systems, particularly glutathione-dependent pathways, which is essential for neutralizing reactive oxygen species (ROS) and protecting neurons from oxidative stress-related excitotoxicity Vitamin D suppresses NF-κB activation and decreases the production toxicity [48-50] Vitamin D strengthens cellular antioxidant capacity by activating redox-regulatory pathways that maintain the GSH/GSSG ratio, a principal indicator of cellular health. Under oxidative stress, GSH detoxifies ROS and reactive nitrogen species (RNS) through conversion to its oxidized form (GSSG), which is subsequently regenerated by glutathione reductase (GR) to preserve redox homeostasis. Vitamin D contributes to increased GSH availability in the brain, which is critical because reduced GSH levels render neurons more vulnerable to ROS accumulation, lipid peroxidation, and membrane damage that may precipitate glutamate-mediated excitotoxicity. Furthermore, elevated GSH levels enhance glutathione peroxidase (GPx) activity, an enzyme directly responsible for reducing hydrogen peroxide (H₂O₂) and lipid peroxides, 2 major sources of neuronal oxidative stress. By augmenting GPx activity and facilitating ROS/RNS detoxification, vitamin D helps disrupt the cascade of oxidative injury that can lead to mitochondrial dysfunction, synaptic impairment, and increased susceptibility to psychiatric disorders. Thus, vitamin D indirectly supports synaptic stability and neuronal integrity by optimizing the GSH pathway [49].
The non-genomic actions of vitamin D are also evident in microglia and across multiple inflammatory cascades. Several studies have reported that Vitamin D attenuates neuroinflammatory signaling by limiting NF-κB activation and reducing the production of proinflammatory cytokines, including IL-6, TNF-α, and IL-1β, in both animal models and cultured brain cells. This mechanism contributes to the attenuation of neuroinflammation, a process widely recognized as central to the pathophysiology of various psychiatric disorders [51-53]. Accordingly, vitamin D may be considered an immunomodulator within the central nervous system, inhibiting the production of proinflammatory cytokines (such as IL-6 and TNF-α) and shifting the immune profile toward a more anti-inflammatory state. This shift substantially reduces chronic neuroinflammation, which is known to play a significant role in the emergence of diverse psychiatric symptoms [54-57].
The role of vitamin D in modulating monoamine neurotransmission further reinforces its relevance to psychiatric symptomatology. Vitamin D influences the regulation of key enzymes involved in serotonin synthesis (including tryptophan hydroxylase-2) and modulates dopaminergic and noradrenergic function in limbic regions, all of which constitute primary targets of antidepressant and antipsychotic medications [54,57,58]. Recent molecular reviews emphasize that vitamin D can enhance serotonin synthesis and release in the brain, stabilize synaptic transmission, and interact with the mechanisms underlying selective serotonin reuptake inhibitors (SSRIs), thereby theoretically reducing antidepressant dose requirements for some patients [58,59]. Beyond the monoaminergic pathway, vitamin D also participates in the regulation of the hypothalamic-pituitary-adrenal (HPA) axis, circadian rhythms, and the neuroendocrine stress system, in which HPA axis dysregulation is strongly associated with increased vulnerability to depression, anxiety, and psychotic symptoms [54,57]. Additionally, the antioxidant effects of vitamin D,mediated through enhancement of total antioxidant capacity and glutathione,help reduce oxidative stress, a feature commonly observed in depressive disorders, psychosis, and chronic substance use [54,56,60].
Overall, the findings of this meta-analysis indicate that vitamin D supplementation is associated with small-to-moderate reductions in psychiatric symptom severity, with the most consistent effects observed in depressive symptoms [61-64]. The biological effects of vitamin D on glutamate-GABA pathways, dopaminergic signaling, and neuroinflammatory regulation appear sufficiently robust to produce measurable improvements in depressive symptoms; however, these mechanisms are likely insufficient to overcome the more complex and chronic circuit dysfunctions characteristic of psychotic disorders, anxiety disorders, and substance use disorders, where long-standing structural and functional abnormalities disrupt brain networks. As a result, clinical effects in these populations tend to be small and inconsistent [65]. At the molecular level, as discussed earlier, vitamin D enhances BDNF and other neurotrophic factors,
increases antioxidant capacity while reducing ROS, and regulates L-type calcium channels and several dopaminergic genes. Nevertheless, these processes operate primarily as fine modulatory adjustments rather than corrective mechanisms capable of reversing aberrant synaptic pruning or longstanding neurodevelopmental alterations observed in psychotic disorders such as schizophrenia and schizoaffective disorder. Thus, although vitamin D exerts biologically protective effects, these are insufficient to overcome entrenched neurodevelopmental damage. Moreover, environmental factors,including social stress, malnutrition, sleep disruption, and physical comorbidities,exert far stronger influences on clinical outcomes than the subtle modulatory actions of vitamin D [65].
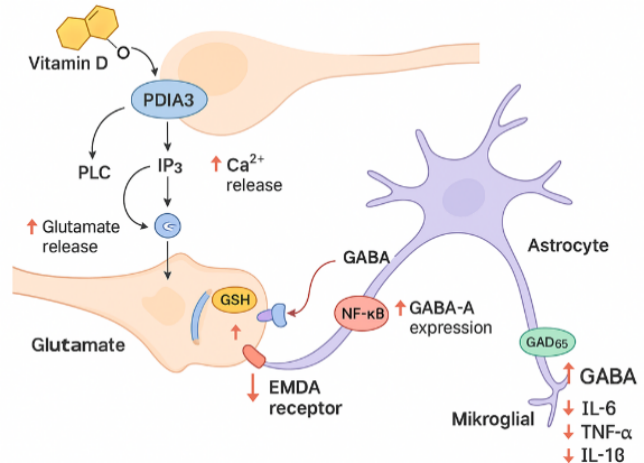
Figure 5 This figure summarizes the non-genomic effects of vitamin D in regulating glutamate–GABA neurotransmission and inflammatory responses. Vitamin D activates PDIA3, triggering the PLC-IP₃ signaling cascade and enhancing Ca²⁺ release, which modulates presynaptic glutamate regulation. In parallel, vitamin D increases glutathione (GSH) levels, thereby reducing oxidative stress and excitotoxicity. Activation of glutamate receptors on microglia is counterbalanced by the vitamin D–mediated suppression of NF-κB, resulting in decreased production of proinflammatory cytokines (IL-6, TNF-α, IL-1β). In astroglial cells, vitamin D upregulates GAD65 activity and GABA-A receptor expression, collectively enhancing inhibitory neurotransmission and restoring excitatory–inhibitory balance. These mechanisms support the role of vitamin D in reducing psychiatric symptoms through the modulation of neuroinflammation, neurotransmission, and neuroprotection. The illustration is original, created based on concepts described in recent literature [40-42].
Regarding anxiety, the molecular explanation for the absence of a significant effect of vitamin D may relate to the distinct neurocircuitry underlying anxiety disorders. Anxiety is predominantly driven by amygdala hyperactivity, heightened noradrenergic signaling, and overactivation of the HPA axis (CRH-ACTH-cortisol). These pathways are not primary targets of vitamin D compared to glutamate-GABA balance and neuroplasticity mechanisms more strongly implicated in depression. Furthermore, many RCTs included populations with mild anxiety symptoms or evaluated “anxiety scores” only as secondary outcomes; therefore, baseline inflammation and synaptic impairment may have been minimal, reducing the likelihood of detecting meaningful clinical effects from vitamin D’s anti-inflammatory actions [66].
In individuals with substance use disorders, depressive symptoms arise through neurobiological mechanisms that overlap substantially with those seen in primary depression. Accordingly, the mechanisms through which vitamin D may reduce depressive symptoms in this population parallel its effects in non-substance-using individuals. Conceptually, vitamin D can modulate the dopaminergic reward pathway (VTA-nucleus accumbens), reduce neuroinflammation, and attenuate oxidative stress, pathophysiological processes that are further exacerbated by addictive substances. Evidence from animal models demonstrates that vitamin D can protect dopaminergic and serotonergic neurons from methamphetamine-induced toxicity [14]. However, in humans with chronic addiction, damage to the reward circuitry, including down-regulation of D2 receptors and long-standing alterations in plasticity within the nucleus accumbens and prefrontal cortex, is often severe and multifactorial, limiting the clinical impact of vitamin D supplementation [67]. Furthermore, existing RCTs in this population tend to involve small sample sizes, short intervention periods, and heterogeneous outcome measures (e.g., metabolic changes, withdrawal symptoms, mood). As a result, when depressive or anxiety symptoms among individuals with substance use disorders are analyzed specifically, effect sizes often fail to reach statistical significance.
The consistency in the overall direction of effect across RCTs and recent meta-analyses strengthens the hypothesis that vitamin D functions as a pharmacological adjuvant targeting shared neurobiological pathways across multiple psychiatric disorders, rather than serving as a primary monotherapy [62,68]. Moreover, clinical benefits appear more pronounced among individuals with low baseline 25(OH)D levels, those receiving moderate-to-high dosing regimens, and studies with sufficiently long follow-up durations. This pattern suggests the presence of a biological “window of opportunity” in which correcting vitamin D deficiency yields the greatest therapeutic relevance for symptom improvement [63,69,70]. These findings align with broader literature indicating that vitamin D deficiency represents a modifiable risk factor across numerous mental health conditions, underscoring the importance of incorporating vitamin D status assessment and correction into the comprehensive management of psychiatric patients [54,56,57].
Conclusions
This meta-analysis demonstrates that vitamin D supplementation is associated with small-to-moderate reductions in psychiatric symptom severity, with the most consistent improvements observed in depressive symptoms. These effects are likely mediated through the modulation of neurotransmission, enhancement of neuroplasticity, suppression of inflammatory pathways, and strengthening of antioxidant defense mechanisms. However, the clinical benefits of vitamin D for anxiety, psychotic symptoms, and substance-related psychiatric manifestations remain inconsistent, likely due to the more complex and chronic neurocircuitry dysfunctions underlying these conditions. Accordingly, vitamin D should be viewed primarily as an adjunctive intervention rather than a stand-alone therapeutic strategy, particularly in individuals with documented deficiency, while evidence for its efficacy in severe psychiatric disorders remains limited. Further large-scale, methodologically rigorous trials are required to clarify optimal dosing strategies, treatment duration, and the specific patient populations most likely to benefit.
Acknowledgements
We did not receive any funding for this research. All contributors in this literature study have been deserved and listed in the authorship.
Declaration of generative AI in scientific writing
The author declares that AI tools were used solely to improve grammar and language clarity, not for content generation, data analysis, or interpretation. The author used biorender and canva applications to make the illustrative graphical abstract. The author reviewed and edited the graphic with full responsibility.
CRediT author statement
Rina Hastuti Lubis: Conceptualization, Methodology, Formal analysis, Data curation, Software, Writing - original draft, Visualization. Hanifah Yusuf: Supervision, Project administration, Writing - review & editing. Khairan Kharian: Data curation, Investigation, Validation, Formal analysis. Nirwana Lazuardi Sary: Resources, Investigation, Methodology, Visualization, Writing - review & editing.
References
M Bellan and P Marzullo. New insights on low vitamin D plasma concentration as a potential cardiovascular risk factor. The Open Rheumatology Journal 2018; 12(1), 261-278.
SE Pratiwi and F Sukmawati. Vitamin D and serotonin’s role in neuropsychiatric disorders. Jurnal Studi Gender dan Anak 2020; 114, 114-128.
L Máčová, R Kancheva and M Bičíková. Molecular regulation of the CNS by vitamin D. Physiological Research 2023; 72(4), S340-S356.
WHO. Over a billion people living with mental health conditions - services require urgent scale-up, Available at: https://www.who.int/news/item/02-09-2025-over-a-billion-people-living-with-mental-health-conditions-services-require-urgent-scale-up, accessed November 2025.
J Liu, W Ning, N Zhang, B Zhu and Y Mao. Estimation of the global disease burden of depression and anxiety between 1990 and 2044: An analysis of the global burden of disease study 2019. Healthcare 2024; 12(17), 1721.
C Kieling, C Buchweitz, A Caye, J Silvani, SH Ameis, AR Brunoni, KT Cost, DB Courtney, K Georgiades, KR Merikangas, JL Henderson, GV Polanczyk, LA Rohde, GA Salum and P Szatmari. Worldwide prevalence and disability from mental disorders across childhood and adolescence: Evidence from the global burden of disease study. JAMA Psychiatry 2024; 81(4), 347-356.
DF Santomauro, AMM Herrera, J Shadid, P Zheng, C Ashbaugh, DM Pigott and C Abbafati. Global prevalence and burden of depressive and anxiety disorders in 204 countries and territories in 2020 due to the COVID-19 pandemic. The Lancet 2021; 398(10312), 1700-1712.
SF Javaid, IJ Hashim, MJ Hashim, E Stip, MA Samad and AA Ahbabi. Epidemiology of anxiety disorders: Global burden and sociodemographic associations. Middle East Current Psychiatry 2023; 30(1), 44.
C Campuzano-Cortina, LM Feijoó-Fonnegra, K Manzur-Pineda, M Palacio-Muñoz, J Rendón-Fonnegra, L Montoya, MC Berrouet and D Restrepo. Comorbidity between depressive symptoms and substance use in-patients hospitalized for non-psychiatric diseases. Revista Colombiana de Psiquiatría 2021; 50(2), 130-137.
JA Puddephatt, P Irizar, A Jones, SH Gage and L Goodwin. Associations of common mental disorder with alcohol use in the adult general population: A systematic review and meta-analysis. Addiction 2022; 117(6), 1543-1572.
RJB Bastien, T Ding, A Gonzalez-Valderrama, L Valmaggia, JB Kirkbride and HE Jongsma. The incidence of non-affective psychotic disorders in low and middle-income countries: A systematic review and meta-analysis. Social Psychiatry and Psychiatric Epidemiology 2023; 58(4), 523-536.
S Ghaemi, S Zeraattalab-Motlagh, A Jayedi and S Shab-Bidar. The effect of vitamin D supplementation on depression: A systematic review and dose-response meta-analysis of randomized controlled trials. Psychological Medicine 2024; 54(12), 3999-4008.
T Mikola, W Marx, MM Lane, M Hockey, A Loughman, S Rajapolvi, T Rocks, A O’Neil, D Mischoulon, M Valkonen-Korhonen, SM Lehto and A Ruusunen. The effect of vitamin D supplementation on depressive symptoms in adults: A systematic review and meta‐analysis of randomized controlled trials. Critical Reviews in Food Science and Nutrition 2023; 63, 11784-11801.
A Ghaderi, M Rasouli-Azad, MH Farhadi, N Mirhosseini, M Motmaen, E Pishyareh, A Omidi, Abdollah and Z Asemi. Exploring the effects of vitamin D supplementation on cognitive functions and mental health status in subjects under methadone maintenance treatment. Journal of Addiction Medicine 2020; 14(1), 18-25.
SA AlGhamdi. Effectiveness of Vitamin D on neurological and mental disorders. Diseases 2024; 12(6), 131.
MJ Page, JE McKenzie, PM Bossuyt, I Boutron, TC Hoffmann, CD Mulrow, L Shamseer, JM Tetzlaff, EA Akl, SE Brennan, R Chou, J Glanville, JM Grimshaw, A Hróbjartsson, MM Lalu, T Li, EW Loder, E Mayo-Wilson and S McDonald. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021; 372, n71.
R DerSimonian and N Laird. Meta-analysis in clinical trials revisited. Contemporary Clinical Trials 2015; 45, 139-145.
JPT Higgins, DG Altman, PC Gøtzsche, P Jüni, D Moher, AD Oxman, J Savović, KF Schulz, L Weeks, JAC Sterne and C Bias. The cochrane collaboration’s tool for assessing risk of bias in randomised trials. BMJ 201; 343(7829), d5928.
JAC Sterne, J Savović, MJ Page, RG Elbers, NS Blencowe, I Boutron, CJ Cates, HY Cheng, MS Corbett, SM Eldridge, JR Emberson, MA Hernán, S Hopewell, A Hróbjartsson, DR Junqueira, P Jüni, JJ Kirkham, T Lasserson, T Li,…, JPT Higgins. RoB 2: A revised tool for assessing risk of bias in randomised trials. The BMJ 2019; 366, 14898.
MA Choukri, TS Conner, JJ Haszard, MJ Harper and LA Houghton. Effect of vitamin D supplementation on depressive symptoms and psychological wellbeing in healthy adult women: A double-blind randomised controlled clinical trial. Journal of Nutritional Science 2018; 7, e23.
S Karami-Mohajeri, S Khalifee, MR Heidari and F Dabaghzadeh. Evaluating the effect of vitamin D3 supplementation on anxiety, depression, sleep quality, and physical morbidity in students of Kerman University of Medical Sciences. Journal of Jiroft University Medical Sciences 2021; 8(3), 709-718.
E Zaromytidou, T Koufakis, G Dimakopoulos, D Drivakou, S Konstantinidou, P Rakitzi, M Grammatiki, E Manthou, A Notopoulos, I Iakovou, A Gotzamani-Psarrakou and K Kotsa. Vitamin D alleviates anxiety and depression in elderly people with prediabetes: A randomized controlled study. Metabolites 2022; 12(10), 884.
A Ghaderi, HR Banafshe, M Motmaen, M Rasouli-Azad, F Bahmani and Z Asemi. Clinical trial of the effects of vitamin D supplementation on psychological symptoms and metabolic profiles in maintenance methadone treatment patients. Progress in Neuro-Psychopharmacology and Biological Psychiatry 2017; 79, 84-89.
F Gaughran, D Stringer and G Wojewodka. Effect of vitamin D supplementation on outcomes in people with early psychosis: The DFEND randomized clinical trial. JAMA Network Open 2021; 4(12), e2140858.
A Krivoy, R Onn, Y Vilner, E Hochman, S Weizman, A Paza, S Hessa, R Sagy, S Kimhi-Neshera, E Kaltera, T Friedmana, Z Friedmana, G Bormanta, S Trommerb, A Valevski and A Weizman. Vitamin D supplementation in chronic schizophrenia patients treated with clozapine: A randomized, double-blind, placebo-controlled clinical trial. EBioMedicine 2017; 26, 138-145.
F Sheikhmoonesi, M Zarghami, S Mamashli, JY Charati, R Hamzehpour, S Fattahi, R Azadbakht, Z Kashi, S Ala, M Moshayedi, H Alinia and N Hendouei. Effectiveness of vitamin D supplement therapy in chronic stable schizophrenic male patients: A randomized controlled trial. Shaheed Beheshti University of Medical Sciences and Health Services Iranian Journal of Pharmaceutical Research 2016; 15(4), 941-950.
F Vellekkatt, V Menon, M Rajappa and J Sahoo. Effect of adjunctive single dose parental vitamin D replacement on improving depression ratings in major depression with concurrent vitamin D deficiency: A double-blind randomized placebo-controlled trial. Journal of Psychiatric Research 2020; 129, 250-256.
JP Hansen, M Pareek, A Hvolby, A Schmedes, T Toft, E Dahl and CT Nielsen. Vitamin D3 supplementation and treatment outcomes in patients with depression (D3-vit-dep). BMC Research Notes 2019; 12(1), 203.
L Libuda, N Timmesfeld, J Antel, R Hirtz, J Bauer, D Führer, D Zwanziger, D Öztürk, G Langenbach, D Hahn, S Ring, T Peters, A Hinney, J Bühlmeier, J Hebebrand, C Grasemann and M Föcker. Effect of vitamin D deficiency on depressive symptoms in child and adolescent psychiatric patients: Results of a randomized controlled trial. European Journal of Nutrition 2020; 59(8), 3415-3424.
MM Kaviani, B Nikooyeh, F Etesam, SJ Behnagh, HM Kangarani, M Arefi, P Yaghmaei and TR Neyestani. Effects of vitamin D supplementation on depression and some selected pro-inflammatory biomarkers: A double-blind randomized clinical trial. BMC Psychiatry 2022; 22(1), 694.
PNS Kumar, V Menon and C Andrade. A randomized, double-blind, placebo-controlled, 12-week trial of vitamin D augmentation in major depressive disorder associated with vitamin D deficiency. Journal of Affective Disorders 2022; 314, 143-149.
PT Satyanarayana, R Suryanarayana, ST Yesupatham, SRV Ramalingareddy and NA Gopalli. Does vitamin D3 supplementation improve depression scores among rural adolescents? a randomized controlled trial. Nutrients 2024; 16(12), 1828.
R Putranto, S Setiati, MW Nasrun, F Witjaksono, S Immanuel, I Subekti, K Harimurti, A Siswanto, H Shatri, S Suwarto and MA Megantara. Effects of cholecalciferol supplementation on depressive symptoms, C-peptide, serotonin, and neurotrophin-3 in type 2 diabetes mellitus: A double-blind, randomized, placebo-controlled trial. Narra J 2024; 4(3), e1342.
ST Rahman, M Waterhouse, BD Romero, C Baxter, DR English, OP Almeida, M Berk, PR Ebeling, BK Armstrong, DSA McLeod, G Hartel, RL O’Connell, H Pham, JG Scott, JC van der Pols, AJ Venn, PM Webb, DC Whiteman and RE Neale. Effect of vitamin D supplementation on depression in older Australian adults. International Journal of Geriatric Psychiatry 2023; 38(1), e5847.
JAC Sterne, AJ Sutton, JPA Ioannidis, N Terrin, DR Jones, J Lau, J Carpenter, G Rücker, RM Harbord, CH Schmid, J Tetzlaff, JJ Deeks, S Duval, DG Altman, D Moher and JPT Higgins. Recommendations for examining and interpreting funnel plot asymmetry in meta-analyses of randomised controlled trials. BMJ 2011; 343(7818), d4002.
M Egger, GD Smith, M Schneider and C Minder. Papers bias in meta-analysis detected by a simple, graphical test. BMJ 1997; 315(7109), 629-634.
B Sailike, Z Onzhanova, B Akbay, T Tokay and F Molnár. Vitamin D in central nervous system: Implications for neurological disorders. International Journal of Molecular Sciences 2024; 25(14), 7809.
BR Kouba and ALS Rodrigues. Neuroplasticity-related effects of vitamin D relevant to its neuroprotective effects: A narrative review. Pharmacology Biochemistry and Behavior 2024; 245, 173899.
J Chen, Y Li, L Wang, Q Liu and B Qiu. Neuroprotective synergy of vitamin D and exercise: a narrative review of preclinical and clinical evidence on aging-related neuroplasticity and cognitive health. Frontiers in Nutrition 2025; 12, 1642363.
MA Żmijewski. Nongenomic activities of vitamin D. Nutrients 2022; 14(23), 5104.
S Donati, G Palmini, C Aurilia, I Falsetti, F Miglietta, T Iantomasi and ML Brandi. Rapid nontranscriptional effects of calcifediol and calcitriol. Nutrients 2022; 14(6), 1291.
J Pietruszkiewicz, K Mrozek, M Zwierz, A Wińska, M Suprunowicz, AJ Oracz and N Waszkiewicz. The neuroprotective potential of vitamin D3. Nutrients 2025; 17(20), 3202.
X Cui and DW Eyles. Vitamin D and the central nervous system: Causative and preventative mechanisms in brain disorders. Nutrients 2022; 14(20), 4353.
DW Eyles. Vitamin D: Brain and behavior. Journal of Bone and Mineral Research Plus 2021; 5(1), e10419.
X Cui and DW Eyles. Vitamin D and the central nervous system: Causative and preventative mechanisms in brain disorders. Nutrients 2022; 14(20), 4353.
L Máčová, R Kancheva and M Bičíková. Molecular regulation of the CNS by vitamin D. Physiological Research 2023; 72, S339-S356.
X Ye, Q Zhou, P Ren, W Xiang and L Xiao. The synaptic and circuit functions of vitamin D in neurodevelopment disorders. Neuropsychiatric Disease and Treatment 2023; 19, 1515-1530.
CA Uthaiah, NC Devaru, NH Shivakumar and SRV Madhunapantula. Vitamin D mitigates hyperglycemia-induced cognition decline in danio rerio (Zebrafish) through the activation of antioxidant mechanisms. Antioxidants 2022; 11(11), 2114.
N Poladian, I Navasardyan, W Narinyan, D Orujyan and V Venketaraman. Potential role of glutathione antioxidant pathways in the pathophysiology and adjunct treatment of psychiatric disorders. Clinics and Practice 2023; 13(4), 768-779.
A Skoczek-Rubińska, A Cisek-Woźniak, M Molska, M Heyser, M Trocholepsza, S Pietrzak and K Mruczyk. Impact of vitamin D status and supplementation on brain-derived neurotrophic factor and mood-cognitive outcomes: A structured narrative review. Nutrients 2025; 17(16), 2655.
AK Fenercioglu. The anti-inflammatory roles of vitamin D for improving human health. Current Issues in Molecular Biology 2024; 46(12), 13514-13525.
N Doncheva, A Mihaylova, H Zlatanova, M Ivanovska, D Delev, M Murdjeva and I Kostadinov. Vitamin D3 exerts immunomodulatory and memory improving properties in rats with lipopolysaccharide-induced inflammation. Folia Medica 2022; 64(5), 770-781.
A Mirarchi, E Albi, T Beccari and C Arcuri. Microglia and brain disorders: The role of vitamin D and its receptor. International Journal of Molecular Sciences 2023; 24(15), 11892.
B Sailike, Z Onzhanova, B Akbay, T Tokay and F Molnár. Vitamin D in central nervous system: Implications for neurological disorders. International Journal of Molecular Sciences 2024; 25(14), 7809. M Almuqbil, ME Almadani, SA Albraiki, AM Alamri, A Alshehri, A Alghamdi, S Alshehri, SMB Asdaq and SMB Asdaq. Impact of vitamin D deficiency on mental health in university students: A cross-sectional study. Healthcare 2023; 11(14), 2097.
AM Ciobanu, C Petrescu, C Anghele, MC Manea, CA Ciobanu, DM Petrescu, MO Antonia and S Riga. Severe vitamin D deficiency-a possible cause of resistance to treatment in psychiatric pathology. Medicina 2023; 59(12), 2056.
HW Baik. Mental health and micronutrients: A narrative review. Annals of Clinical Nutrition and Metabolism 2024; 16(3), 112-119.
ZZ Bostan, MŞ Bulut and MG Karadağ. Can vıtamın D reduce the need for SSRI by modulatıng serotonın synthesıs?: A revıew of recent lıterature. Current Nutrition Reports 2025; 14(1), 1-12.
Ş Akpınar and MG Karadağ . Is vitamin D important in anxiety or depression? What is the truth? Current Nutrition Reports 2022; 11(4), 675-681.
A Ghaderi, HR Banafshe, M Motmaen, M Rasouli-Azad, F Bahmani and Z Asemi. Clinical trial of the effects of vitamin D supplementation on psychological symptoms and metabolic profiles in maintenance methadone treatment patients. Progress in Neuro-Psychopharmacology and Biological Psychiatry 2017; 79, 84-89.
SA AlGhamdi. Effectiveness of vitamin D on neurological and mental disorders. Diseases 2024; 12(6), 131.
ML Raza, ST Hassan, S Jamil, W Fatima and M Fatima. Nutritional interventions in depression: The role of vitamin D and omega-3 fatty acids in neuropsychiatric health. Clinical Nutrition 2025; 45, 270-280.
D Guzek, A Kołota, K Lachowicz, D Skolmowska, M Stachoń and D Głąbska. Effect of vitamin D supplementation on depression in adults: A systematic review of Randomized Controlled Trials (RCTs). Nutrients 2023; 15(4), 951.
J Fu, Y Zhang, X Chen, X Yu, M Yan, B Jing, H Yu, W Li and Q Guo. Efficacy of vitamin D supplementation on depressive symptoms in older patients: a meta-analysis of randomized controlled trials. Frontiers in Medicine 2024; 11, 1467234.
J Tsiglopoulos, N Pearson, N Mifsud, K Allott and B O’Donoghue. The association between vitamin D and symptom domains in psychotic disorders: A systematic review. Schizophrenia Research 2021; 237, 79-92.
LOL Centeno, MS Fernandez, FWMG Muniz, A Longoni and AM de Assis. Is serum vitamin D associated with depression or anxiety in ante- and postnatal adult women? a systematic review with meta-analysis. Nutrients 2024; 16(21), 3648.
J García-Estrada, S Luquin, K Pesqueda-Cendejas, AI Ruiz-Ballesteros, B Campos-López, MR Meza-Meza, I Parra-Rojas, RE González-Castañeda, O Ramos-Lopez and UD la Cruz-Mosso. Malnutrition in substance use disorders: A critical issue in their treatment and recovery. Healthcare 2025; 13(8), 868.
T Mikola, W Marx, MM Lane, M Hockey, A Loughman, S Rajapolvi, T Rocks, A O’Neil, D Mischoulon, M Valkonen-Korhonen, SM Lehto and A Ruusunen. The effect of vitamin D supplementation on depressive symptoms in adults: A systematic review and meta‐analysis of randomized controlled trials. Critical Reviews in Food Science and Nutrition 2023; 63(33), 11784-11801.
S Ghaemi, S Zeraattalab-Motlagh, A Jayedi and S Shab-Bidar. The effect of vitamin D supplementation on depression: A systematic review and dose-response meta-analysis of randomized controlled trials. Psychological Medicine 2024; 54(15), 3999-4008.
Y Park, YM Ah and YM Yu. Vitamin D supplementation for depression in older adults: A meta-analysis of randomized controlled trials. Frontiers in Nutrition 2023; 10, 1169436.