Trends
Sci.
2026;
23(9):
12853
Combined Effects of Sacha Inchi Protein Hydrolysate and Reduced-Dose Captopril on Duodenal and Cecal Morphology in L-NAME-Induced Hypertensive Rats
Jarinthorn Teerapornpuntakit1, Tippaporn Bualeong2, Pakaporn Sa-nguanpong2,
Worasit Tochampa3, Khanitta Ruttarattanamongkol3, Supawadee Auten4,
Pornpichaya Yottue4, Papichaya Bournoi4, Pattarawadee Sawangwong4,
Hiroki Nakata5, Yutthapong Tongpob6,7 and Charkriya Promsuban6,7,*
1Physiology Division, Preclinical Science, Faculty of Medicine, Thammasat University, Pathum Thani 12120, Thailand
2Department of Physiology, Faculty of Medical Science, Naresuan University, Phitsanulok 65000, Thailand
3Department of Agro-Industry, Faculty of Agriculture, Natural Resources and Environment, Naresuan University, Phitsanulok 65000, Thailand
4Faculty of Medical Science, Naresuan University, Phitsanulok 65000, Thailand
5Department of Clinical Engineering, Faculty of Health Sciences, Komatsu University, Komatsu 923-0946, Japan
6Department of Anatomy, Faculty of Medical Science, Naresuan University, Phitsanulok 65000, Thailand
7Center of Excellence in Medical Biotechnology, Faculty of Medical Science, Naresuan University,
Phitsanulok 65000, Thailand
(*Corresponding author’s e-mail: [email protected])
Received: 30 November 2025, Revised: 28 December 2025, Accepted: 5 January 2026, Published: 25 March 2026
Abstract
Hypertension disrupts intestinal homeostasis through structural remodeling and immune activation, contributing to gastrointestinal pathology. Angiotensin-converting enzyme inhibition confers measurable but incomplete tissue protection, suggesting that adjunctive approaches may further preserve intestinal integrity. This exploratory experimental study examined the intestinal effects of captopril alone or in combination with Sacha inchi protein hydrolysate, a plant-derived protein powder obtained from Plukenetia volubilis, in L-NAME-induced hypertensive rats (n = 4 - 5 per group). Animals were allocated to control, L-NAME, L-NAME plus captopril (5 mg/kg), or L-NAME plus low-dose captopril (2.5 mg/kg) combined with Sacha inchi protein hydrolysate (500 mg/kg). Histological analyses of the duodenum and cecum showed that L-NAME treatment induced pronounced mucosal thinning, muscular hypertrophy, reduced collagen deposition, vascular dilation, and increased inflammatory cell infiltration. Full-dose captopril partially attenuated these alterations but did not fully restore intestinal architecture. In contrast, the combination treatment significantly increased mucosal thickness in both intestinal regions (p < 0.001), enhanced collagen deposition (p < 0.05), and improved vascular architecture (p < 0.05), while inflammatory indices showed a consistent trend toward reduction. For several parameters, the combined regimen achieved outcomes comparable to or exceeding those observed with full-dose captopril. Collectively, these findings indicate that Sacha inchi protein hydrolysate may augment the intestinal protective effects of captopril under hypertensive conditions. Although preliminary and limited by sample size, the results provide supportive evidence for further investigation of plant-derived bioactive proteins as adjunctive strategies to mitigate hypertension-associated gastrointestinal remodeling.
Keywords: Captopril, Hypertension model, Intestinal histology, Mucosal remodeling, Inflammation, Sacha inchi protein hydrolysate, L-NAME
Introduction
Hypertension affects over 1.13 billion people worldwide and represents a major risk factor for cardiovascular diseases, contributing significantly to global morbidity and mortality [1]. Beyond its well-established cardiovascular effects, mounting evidence indicates that hypertension induces pathological changes in multiple organ systems. In recent years, increasing attention has focused on the gastrointestinal tract as a secondary target organ, given its high vascularization, immune activity, and sensitivity to hemodynamic and inflammatory disturbances. Hypertension has been shown to disrupt intestinal barrier integrity, alter mucosal perfusion, and promote local immune activation, thereby contributing to systemic inflammation and disease progression [2]. These gut alterations are increasingly recognized as part of a bidirectional gut-vascular-immune axis that may influence blood pressure regulation and cardiovascular risk. One widely used model for studying hypertension in experimental animals is the Nω-Nitro-L-arginine methyl ester (L-NAME)-induced hypertensive rat model, which mimics endothelial dysfunction by inhibiting nitric oxide synthase, leading to elevated blood pressure and oxidative stress [3-5]. Importantly, nitric oxide deficiency also compromises intestinal blood flow and mucosal defense mechanisms, making this model particularly relevant for investigating hypertension-associated gut pathology.
Captopril, an angiotensin-converting enzyme (ACE) inhibitor, is widely used in the management of hypertension and has well-established therapeutic benefits in heart failure, diabetic nephropathy, and cardiovascular risk reduction, largely through modulation of the renin-angiotensin-aldosterone system and improvement of endothelial function [6]. In experimental models, captopril effectively lowers blood pressure and attenuates L-NAME–induced vascular injury. Notably, a reduced dose of captopril (2.5 mg/kg) has also been reported to exert antihypertensive effects, supporting its use in dose-reduction paradigms [3,7]. However, captopril therapy is associated with several clinically relevant adverse effects, including persistent dry cough, hyperkalemia, hypotension, skin reactions, and, in rare cases, angioedema. These limitations have prompted continued research into complementary strategies that may preserve therapeutic efficacy while reducing drug exposure and potential side effects [8].
Accordingly, combination approaches that allow partial dose reduction of conventional antihypertensive agents while maintaining biological effectiveness are of growing interest. Plant-derived bioactive compounds represent promising complementary agents due to their generally favorable safety profiles and diverse biological activities. Sacha inchi (Plukenetia volubilis L.), a plant native to the Amazon region and increasingly cultivated in Southeast Asia, is known for its high content of essential fatty acids, antioxidants, and bioactive proteins [9]. Emerging studies have suggested that protein hydrolysates from Sacha inchi may exhibit ACE-inhibitory activity, antioxidant properties, and vascular-protective effects [10]. The oral dose of 500 mg/kg used in the present study was selected based on prior reports demonstrating biological efficacy and safety of Sacha inchi–derived protein hydrolysates and peptides at comparable doses in rodent models [3]. However, their potential role as adjunctive agents to pharmaceutical ACE inhibitors, particularly in preserving intestinal structure under hypertensive conditions, has not been systematically explored.
The small intestine, particularly the duodenum, plays a crucial role in nutrient absorption and immune surveillance. Structural components such as villi and crypts increase the absorptive surface area, while lymphoid structures like Peyer's patches contribute to mucosal immunity [11]. Hypertension-associated alterations in these features - including villus remodeling, extracellular matrix disruption, and inflammatory infiltration - may compromise barrier integrity and amplify systemic inflammatory signaling [12]. Similarly, the cecum, part of the large intestine, harbors a diverse microbial community and lymphoid tissue, contributing to immune modulation and metabolic processes [13]. Hypertension can induce morphological alterations in these structures, including villus atrophy, increased inflammatory cell infiltration, and changes in mucosal architecture, which may contribute to systemic inflammation and disease progression [14]. For instance, studies have documented increased villus length and mucosal thickness in response to various stimuli, reflecting hyperplasia of cellular elements. Moreover, the presence and organization of lymphoid nodules, such as Peyer's patches, are vital for initiating immune responses and maintaining gut homeostasis [15]. Disruptions in these structures may contribute to systemic inflammation and hypertension.
Despite growing recognition of gut–cardiovascular interactions, the intestinal histopathological consequences of combining conventional antihypertensive therapy with functional food-derived bioactive compounds remain poorly characterized. In particular, whether adjunctive plant-derived proteins can preserve intestinal architecture and immune balance while enabling partial dose reduction of ACE inhibitors has not been adequately investigated.
Therefore, this study was designed to test the hypothesis that Sacha inchi protein hydrolysate enhances the intestinal protective effects of captopril by improving mucosal structure, extracellular matrix integrity, vascular morphology, and immune cell profiles under hypertensive conditions. In addition to their reported ACE-inhibitory and antioxidant activities, plant-derived low–molecular weight protein hydrolysates may interact with the intestinal microenvironment, potentially influencing local drug stability, tissue exposure, or mucosal responses, although pharmacokinetic and physicochemical parameters were not directly assessed in this study. A reduced captopril dose (2.5 mg/kg), previously reported to exert submaximal antihypertensive effects, was therefore selected to evaluate whether combination therapy could achieve intestinal protection comparable to or exceeding that of standard-dose monotherapy. Using the L-NAME-induced hypertension model, this exploratory dose-reduction approach aimed to provide mechanistic and translational insight into combination strategies for mitigating hypertension-associated gastrointestinal remodeling.
Materials and methods
Study design and ethical approval
This study employed a randomized controlled experimental design to investigate the protective effects of captopril and Sacha inchi protein hydrolysate on intestinal histological changes in L-NAME-induced hypertension. The study protocol was approved by the Institutional Animal Care and Use Committee (IACUC) of the Center for Animal Research, Naresuan University (Protocol No. NU-AE650813), and conducted in strict accordance with the National Institutes of Health Guidelines for the Care and Use of Laboratory Animals.
Animal and study design
Adult male Sprague Dawley rats (6 weeks old, weighing 200 - 250 g) were obtained from Nomura Siam International (Thailand). All animals were acclimatized for one week before experimental procedures, and housed individually under standard laboratory conditions (temperature 22 ± 2 °C, relative humidity 50% - 60%, and 12-hour light/dark cycle) with ad libitum access to standard chow and water.
Sample size determination and statistical considerations
Sample size estimation was performed using G*Power 3.1.9.7 software based on preliminary histological measurements of intestinal mucosal thickness obtained from pilot experiments and effect sizes reported in previous studies using L-NAME-induced hypertensive models. An anticipated large effect size (Cohen’s d = 1.2) was applied, reflecting the magnitude of mucosal alterations observed in preliminary analyses rather than an arbitrarily selected value, with an α-error probability of 0.05 and a desired statistical power of 0.80. Under these assumptions, the minimum required sample size was calculated as n = 4 animals per group. To reduce the impact of potential attrition and to improve the robustness of group-level comparisons, group sizes were increased to n = 4 - 5 animals where feasible (total n = 19). Given the small sample size, this study was designed as an exploratory investigation, and statistical power should be interpreted with appropriate caution. No animals were lost during the experimental period.
Experimental groups and treatment protocol
After a 1-week acclimatization period, rats were randomly allocated to experimental groups using a computer-generated randomization sequence. Rats were randomly assigned to four experimental groups (n = 4 - 5 per group): Group 1 (Control): Normal rats receiving distilled water (vehicle) orally once daily; Group 2 (L-NAME): Rats receiving L-NAME at a dose of 40 mg/kg/day dissolved in distilled water and administered by oral gavage once daily for 5 weeks to induce hypertension; Group 3 (L-NAME + captopril): hypertensive rats receiving captopril at 5 mg/kg/day dissolved in distilled water by oral gavage once daily for 5 weeks; and Group 4 (L-NAME + captopril + Sacha inchi): hypertensive rats receiving low-dose captopril (2.5 mg/kg/day) combined with Sacha inchi protein hydrolysate (500 mg/kg/day), both freshly prepared in distilled water and administered by oral gavage once daily for 5 weeks. All treatments were administered via oral gavage using a blunt-tipped feeding needle (18-gauge, 3-inch length) at consistent time points (08:00 - 09:00 am) to minimize circadian variations. All solutions were prepared fresh daily, and dosing volumes were adjusted according to individual body weight. Treatment volumes were standardized at 1 mL/kg body weight across all groups. Control animals underwent identical oral gavage procedures with vehicle alone, serving as sham-treated controls for handling and administration stress.
Blood pressure monitoring
Systolic blood pressure measurements were performed weekly using an indirect tail-cuff system (ML 125 NIBP system, AD Instruments, Sydney, Australia) and were monitored throughout the 5-week study using a PowerLab recording system (AD Instruments, Sydney, Australia), following acclimatization of animals to the procedure, as previously described. Blood pressure measurements were conducted concurrently with the present study using identical experimental conditions and protocols to those reported in our previously published work [3]. These measurements confirmed successful induction of hypertension in L-NAME-treated rats and demonstrated comparable reductions in systolic blood pressure between the full-dose captopril group (5 mg/kg) and the low-dose captopril plus Sacha inchi protein hydrolysate group (2.5 mg/kg), thereby supporting the rationale for examining intestinal outcomes under conditions of similar blood pressure control.
Preparation of Sacha inchi protein hydrolysate
Sacha inchi protein hydrolysate was prepared according to our previously established protocol [3]. Briefly, the seed cake was ground and sieved through a 60-mesh screen, then combined with water at a 1:5 ratio to extract protein and obtain a protein isolate. The pH was adjusted to 9 with 1 M sodium hydroxide, followed by incubation at 45 °C for one hour. After centrifugation, the protein was precipitated by lowering the pH to 4.5 using 1 M hydrochloric acid, and the precipitate was subsequently freeze-dried. For hydrolysis, the protein isolate was reconstituted in water, and the pH was adjusted to 6.5. Alcalase® 2.4 L (2.4 AU-A/g, 1%; Novozymes, Denmark) was added to facilitate enzymatic hydrolysis at 40 °C. The reaction was terminated by heating the mixture to 95 °C for 15 min, followed by centrifugation. The final hydrolysate was freeze-dried and stored at –20 °C to obtain powdered Sacha inchi protein hydrolysate.
Sample collection and histological processing
Duodenal and cecal tissues were collected from all rats. These samples were fixed in 10% neutral-buffered formalin for 7 days. Following fixation, the tissue specimens were processed and embedded in paraffin wax. Paraffin-embedded tissue blocks were then sectioned at a thickness of 3 µm using a rotary microtome. Two staining protocols were performed on the tissue sections: Hematoxylin and eosin (H&E) staining for general morphological assessment, and Masson’s Trichrome staining for collagen fiber visualization. All staining procedures followed standardized protocols with appropriate positive and negative controls included in each batch. Each slide was scanned and captured at three representative fields of view using the Aperio ImageScope software (version 10.0.35.1798).
Histomorphometric analysis
Histological characteristics of both duodenal and cecal tissues were examined under a light microscope in three non-overlapping fields per section. Field selection was performed using a predefined systematic approach to minimize selection bias. Briefly, each section was initially scanned at low magnification (4× - 10×) to identify well-oriented regions with intact mucosal architecture. Three fields were then selected from the central region of each section, avoiding areas with tissue folds, tears, edge artifacts, or obvious processing damage. All field selection and quantitative analyses were conducted by investigators blinded to experimental group allocation. For H&E-stained sections, both morphological and quantitative assessments were conducted. Measurements included the thickness of the intestinal wall layers - mucosa, submucosa, and muscularis externa, and the area of lymphoid tissues within the mucosa - at 40× magnification. At 100× magnification, the height and width of intestinal villi in the duodenum and the depth and width of intestinal glands in the cecum were evaluated. In addition, the number of inflammatory cells and the number of goblet cells within the mucosa were quantified at 100× magnification. The diameter of blood vessels within the submucosal layer of both the duodenum and cecum was also measured at 100×. Moreover, the structural features of the crypts of Lieberkühn in the mucosal layer were examined at the same magnification. For Masson’s Trichrome-stained sections, quantitative analysis focused on measuring the collagen area within the intestinal wall layers - mucosa, submucosa, and muscularis externa - using a 40× objective lens. All quantitative data were analyzed using the ImageJ software. To ensure measurement reliability, 20% of images were randomly selected and re-analyzed by the same investigator after a 2-week interval (intra-observer reliability) and by a second independent investigator blinded to treatment groups (inter-observer reliability). Intra-class correlation coefficients exceeded 0.85 for all measurements, confirming acceptable reproducibility.
Statistical analysis
Statistical analyses were performed using GraphPad Prism 9 (GraphPad Software Inc., CA, USA). Parametric data were analyzed using one-way analysis of variance (ANOVA) followed by Tukey’s multiple comparison test to adjust for multiple pairwise comparisons and control the family-wise error rate. Data are presented as mean ± standard error of the mean (SEM). Statistical significance was defined as p < 0.05 after Tukey’s post hoc adjustment. To complement p-value-based inference, effect sizes were calculated and reported for key outcomes. Eta-squared (η²) was used to estimate the proportion of variance explained by group effects in ANOVA, while Cohen’s d was calculated for selected pairwise comparisons to quantify the magnitude of differences between treatment groups. Given the exploratory design and limited sample size, effect size estimates were included to aid interpretation of biological relevance beyond statistical significance.
Results and discussion
Dose-sparing effects on intestinal (both duodenal and cecal) wall architecture in L-NAME-induced hypertensive rats
Representative histological images of duodenum and cecum demonstrated clear morphological differences between treatment groups (Figure 1). In the duodenum, the combination therapy group (Group 4: L-NAME + captopril + Sacha inchi) achieved significantly greater mucosal thickness compared to both control and L-NAME groups (p < 0.001 and p < 0.05, respectively; Figure 2(A)). The stronger statistical difference relative to control reflects mucosal thickness values exceeding baseline levels, whereas the comparison with the L-NAME group represents recovery from hypertension-induced injury. Direct comparison between Group 4 and full-dose captopril monotherapy (Group 3) revealed no significant difference, indicating comparable effects on mucosal thickness despite the reduced captopril dose. The submucosal thickness of duodenum in the captopril monotherapy group (Group 3: L-NAME + captopril) was significantly increased compared to control (p < 0.01; Figure 2(B)), while the combination therapy (Group 4) demonstrated a notable protective effect on muscularis externa, showing significantly reduced thickness compared to both L-NAME and captopril monotherapy groups (p < 0.05 and p < 0.01, respectively; Figure 2(C)), suggesting attenuation of hypertension-associated smooth muscle hypertrophy rather than generalized wall thickening.
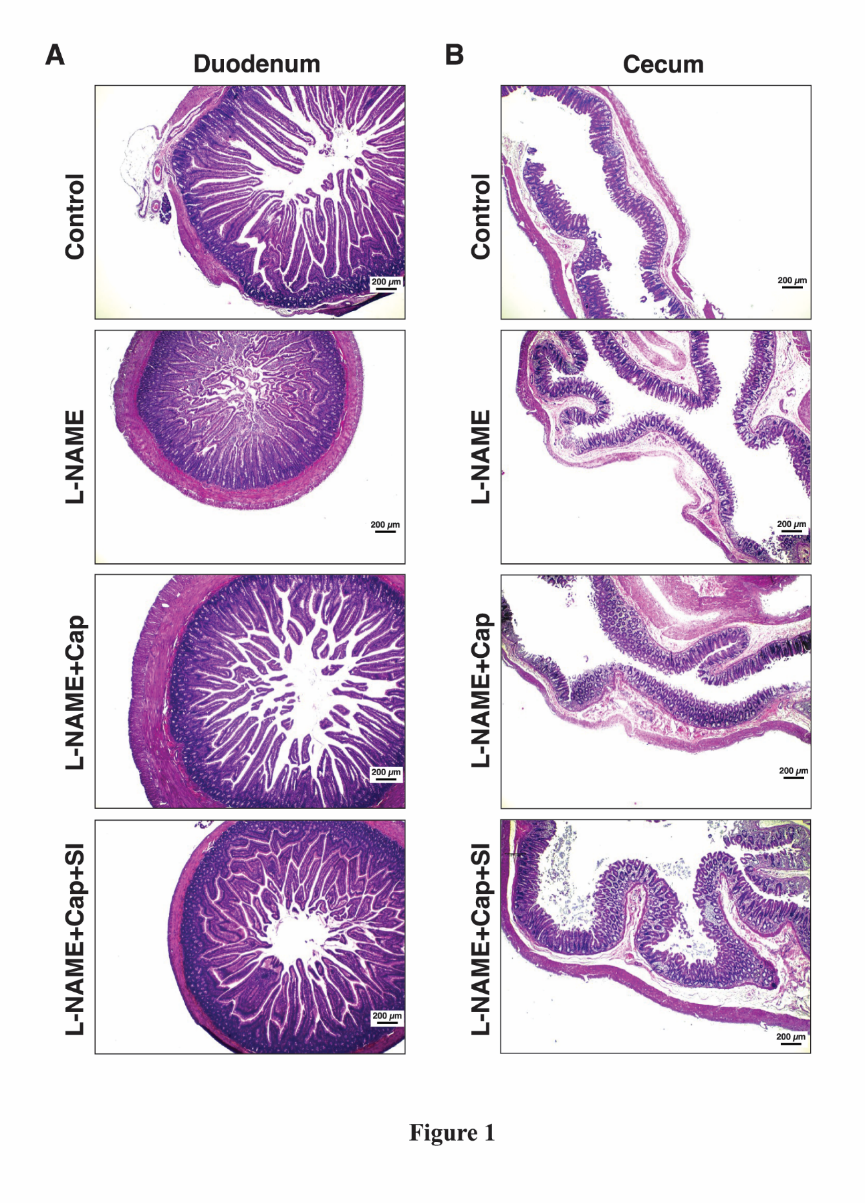
Figure 1 Representative histological images of the intestinal wall illustrating the mucosa, submucosa, and muscularis externa. (A) Duodenal tissue sections; (B) Cecal tissue sections. Images were obtained from animals in the L-NAME, L-NAME + captopril, and L-NAME + captopril + Sacha inchi protein hydrolysate groups using a 40× microscope objective. LN: L-NAME, Cap: captopril, SI: Sacha inchi protein hydrolysate.
In the cecum, similar dose-sparing effects were observed. The combination therapy group (Group 4) showed significantly increased mucosal thickness compared to control and L-NAME groups (p < 0.001 and p < 0.05, respectively; Figure 2(D)). Comparison between Groups 3 and 4 revealed no statistically significant difference in mucosal thickness, supporting comparable structural outcomes between full-dose captopril and the reduced-dose combination regimen. The submucosal layer in Group 4 was significantly thicker than in the captopril monotherapy group (p < 0.001; Figure 2(E)), indicating region-specific structural modulation associated with the combined treatment. Conversely, the L-NAME group exhibited significantly thinner muscularis externa compared to both control and captopril groups (p < 0.05; Figure 2(F)), potentially reflecting structural deterioration under hypertensive conditions.
==
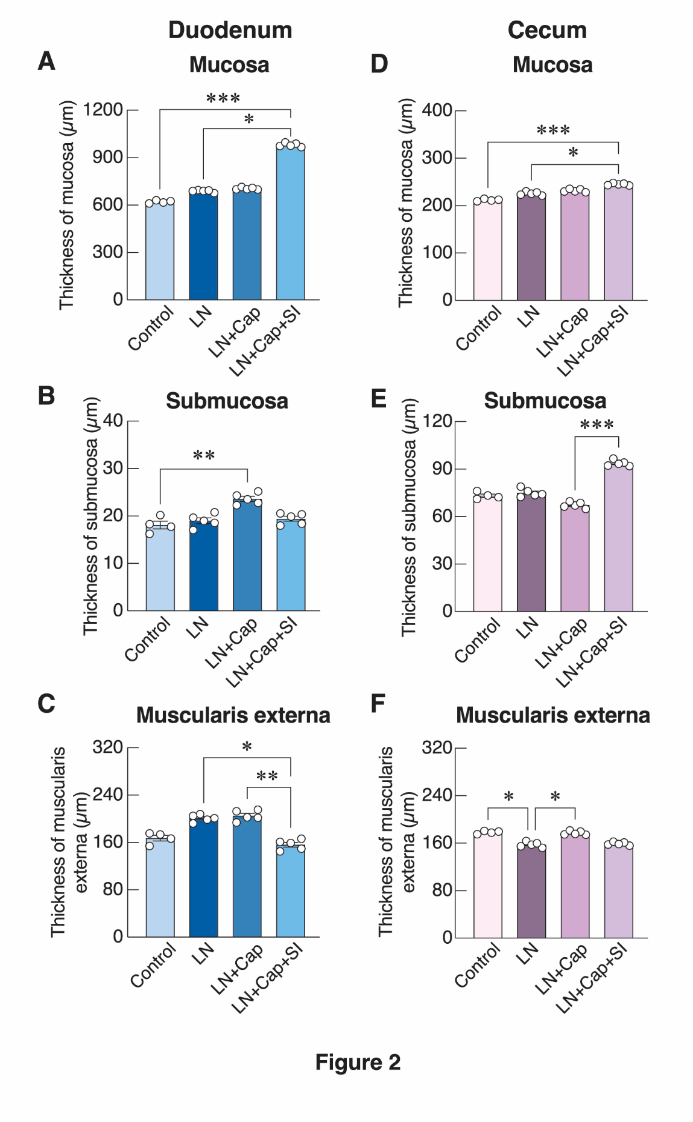
Figure 2 Quantitative analysis of intestinal wall thickness in different segments. (A-C) Duodenum: thickness of the mucosa (A), submucosa (B), and muscularis externa (C). (D-F) Cecum: Thickness of the mucosa (D), submucosa (E), and muscularis externa (F) in the control, L-NAME, L-NAME + captopril, and L-NAME + captopril + Sacha inchi protein hydrolysate. LN: L-NAME, Cap: captopril, SI: Sacha inchi protein hydrolysate. Data are expressed as mean ± S.E.M. Statistical significance among the four experimental groups is indicated as follows: *p < 0.05, **p < 0.01, and ***p < 0.001.
This study demonstrates that combining Sacha inchi protein hydrolysate with a reduced dose of captopril effectively mitigates intestinal structural deterioration in L-NAME-induced hypertensive rats. The improvements observed in both duodenal and cecal morphology indicate a clear dose-sparing benefit that parallels, and in some parameters exceeds, the effects of full-dose captopril monotherapy. Hypertension induced by nitric oxide deficiency is known to impair intestinal structure through ischemia, oxidative stress, and inflammatory activation [16]. Consistent with these mechanisms, the L-NAME group in our study exhibited mucosal thinning, altered submucosal integrity, and muscularis abnormalities. Captopril partially restored these changes, aligning with previous evidence that ACE inhibition improves microcirculation and reduces local inflammation [17]. Importantly, the combination therapy produced a more robust protective effect. Mucosal thickness in the duodenum and cecum was significantly improved, reaching levels comparable to or greater than those achieved with full-dose captopril. Enhanced submucosal thickness in the cecum further suggests improved extracellular matrix remodeling or vascular support, whereas attenuation of muscularis externa thickening in the duodenum points to a modulatory effect on smooth muscle hypertrophy - features commonly associated with hypertensive remodeling. These findings imply that Sacha inchi protein hydrolysate may exert complementary biological activities, potentially through antioxidant, anti-inflammatory, or barrier-protective mechanisms reported in other plant-derived bioactive peptides [3,18,19]. By enhancing tissue restoration while allowing a reduced captopril dose, the combination therapy supports a dose-sparing strategy that may reduce long-term drug burden without compromising protective efficacy.
Enhanced intestinal gland epithelial architecture with combination therapy
Representative images of the intestinal glands (Crypts of Lieberkühn) in the duodenum and cecum were shown in Figures 3(A) and 4(A). The morphology of the intestinal glands (duodenal villus depth, duodenal villus height, cecal gland depth and cecal gland width) was assessed across all experimental groups. In the duodenum, the villus depth in Group 4 (L-NAME + captopril + Sacha inchi protein hydrolysate) was significantly greater than in control and L-NAME (p < 0.001 and p < 0.05, respectively; Figure 3(B)), indicating enhanced mucosal remodeling. Interestingly, duodenal villus height was significantly reduced in the combination group compared to captopril monotherapy (p < 0.001; Figure 3(C)), suggesting distinct architectural remodeling patterns.
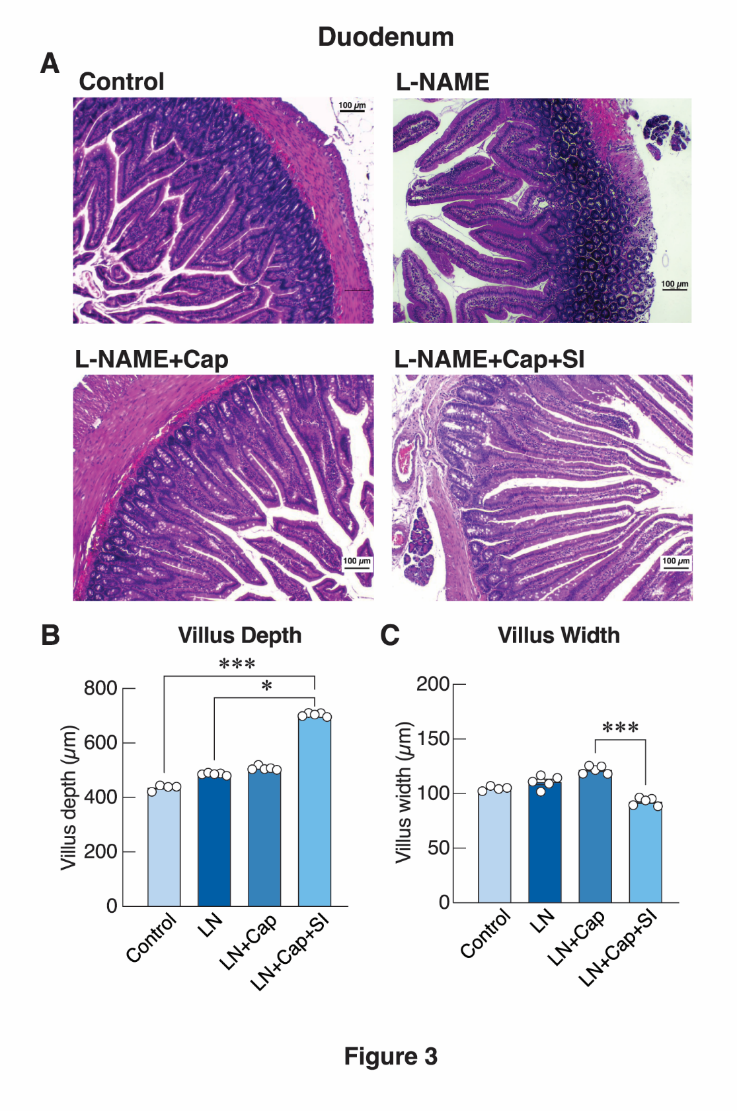
Figure 3 Histological and quantitative analysis of duodenal villi. (A) Representative histological images of the duodenal villi showing villus depth and width in the control, L-NAME, L-NAME + captopril, and L-NAME + captopril + Sacha inchi protein hydrolysate groups. Images were captured using a 100× microscope objective. (B) Quantitative measurements of villus depth in the duodenal wall. (C) Quantitative measurements of villus width in the duodenal wall. LN: L-NAME, Cap: Captopril, SI: Sacha inchi protein hydrolysate. Data are presented as mean ± S.E.M. Statistical significance among the 4 experimental groups is indicated as follows: *p < 0.05, and ***p < 0.001.
In the cecum, captopril monotherapy significantly increased intestinal gland (crypt) depth compared to both control and hypertension (p < 0.001 and p < 0.05, respectively; Figure 4(B)), with cecal glandular width also significantly increased compared to control (p < 0.05; Figure 4(C)), indicating a proliferative response following captopril treatment.
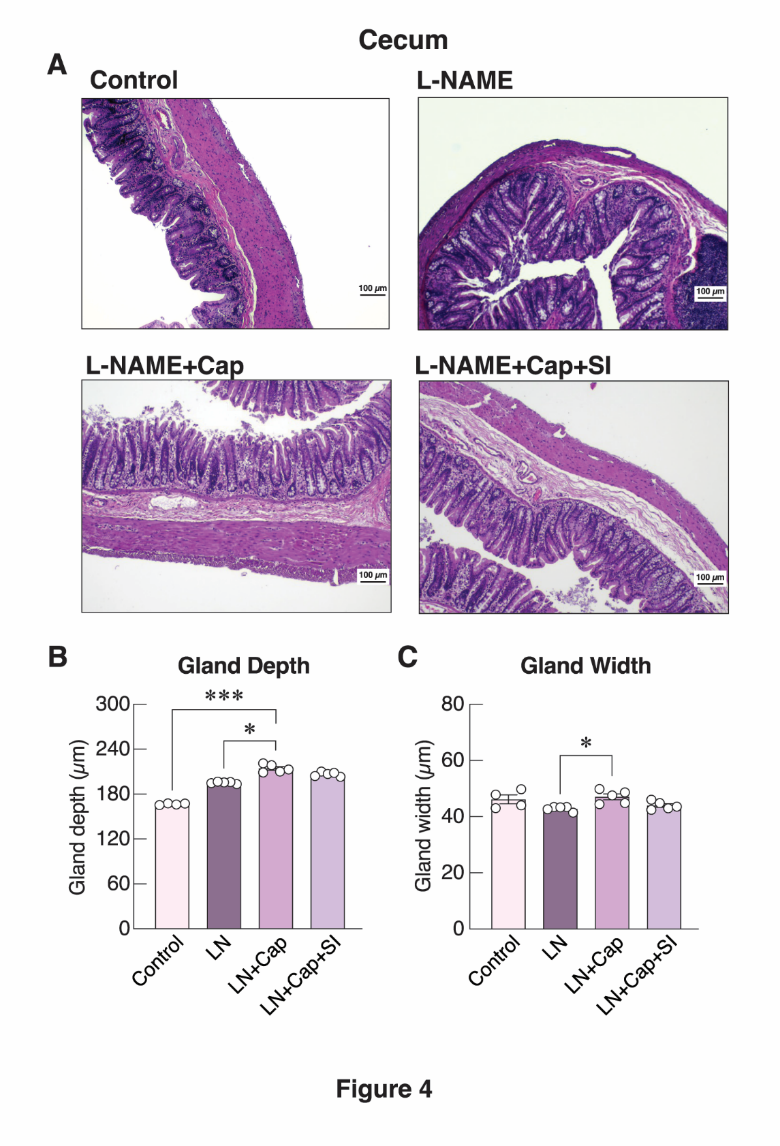
Figure 4 Histological and quantitative analysis of intestinal glands in the cecal wall. (A) Representative histological images showing intestinal gland depth and width in the control, L-NAME, L-NAME + captopril, and L-NAME + captopril + Sacha inchi protein hydrolysate groups. Images were captured using a 100× microscope objective. (B) Quantitative measurements of intestinal gland depth in the cecal wall. (C) Quantitative measurements of intestinal gland width in the cecal wall. LN: L-NAME, Cap: captopril, SI: Sacha inchi protein hydrolysate. Data are presented as mean ± S.E.M. Statistical significance among the four experimental groups is indicated as follows: *p < 0.05, and ***p < 0.001
The present findings reveal distinct patterns of intestinal gland remodeling in both the duodenum and cecum among hypertensive rats receiving reduced-dose captopril combined with Sacha inchi protein hydrolysate. In the duodenum, the combination therapy significantly increased villus depth compared with control and hypertensive groups, indicating enhanced mucosal regeneration and deepening of the crypt-villus axis. This deeper villus interface suggests improved epithelial turnover and potentially enhanced absorptive capacity, consistent with previous evidence that bioactive peptides may stimulate crypt cell proliferation and mucosal repair [17,20]. Interestingly, villus height was reduced in the combination therapy group compared with captopril monotherapy, suggesting a differential architectural remodeling pattern. Shorter villi with deeper crypts may reflect a shift toward increased epithelial renewal or early-stage mucosal restructuring rather than overt villus elongation. Such an arrangement has been described in conditions of active mucosal recovery, where crypt hyperplasia precedes villus height restoration [12]. This pattern may also indicate that the combined treatment modulates epithelial turnover differently from captopril alone, potentially through antioxidant or immunomodulatory actions. In the cecum, captopril monotherapy alone produced a notable increase in both crypt depth and glandular width, demonstrating a proliferative response within the glandular epithelium. These changes may reflect improved microcirculation and reduced inflammatory burden in the cecal mucosa, consistent with known ACE inhibitor effects on intestinal vascular and immune function [21]. The expansion of glandular structures could also indicate enhanced epithelial renewal - an adaptive response counteracting hypertension-induced mucosal stress. Regarding villus and crypt architecture, the observed reduction in villus height accompanied by increased villus depth and crypt dimensions in certain treatment groups may reflect adaptive remodeling rather than complete restoration. Because proliferative activity was not directly assessed, these architectural changes should be interpreted cautiously, and future studies incorporating epithelial proliferation markers (e.g., Ki67) will be required to distinguish regenerative from maladaptive responses. Collectively, these observations suggest that while captopril promotes cecal glandular proliferation, the addition of Sacha inchi protein hydrolysate produces a more nuanced remodeling effect in the duodenum, emphasizing deeper but shorter villi. These differences highlight region-specific responses within the gastrointestinal tract and underscore the potential of bioactive plant peptides to modulate epithelial architecture in ways that complement pharmacological therapy. Further molecular analyses of epithelial proliferation markers and crypt stem cell activity would help clarify the mechanisms underlying these distinct remodeling patterns.
Vascular remodeling and microcirculatory effects of combination therapy
Vascular analysis revealed region-specific responses to treatment. The diameters of blood vessels in the duodenal and cecal walls were evaluated to assess vascular changes associated with hypertension and the effects of treatment. The representative images were shown in Figures 5(A) and 5(B). In the duodenum, L-NAME treatment significantly increased vessel diameter compared to control (p < 0.001; Figure 5(C)), consistent with hypertension-associated vascular dilation. In the context of nitric oxide synthase inhibition, this enlargement likely reflects maladaptive remodeling driven by endothelial dysfunction and sustained hemodynamic stress rather than improved perfusion.
In contrast, the cecal microvasculature exhibited a distinct response pattern. Combination therapy resulted in a significantly greater vessel diameter compared to the L-NAME group (p < 0.05; Figure 5(D)). Importantly, this increase occurred relative to hypertensive animals rather than controls, suggesting a treatment-associated vascular response rather than primary pathological dilation. In this context, increased vessel diameter may reflect adaptive or compensatory remodeling aimed at improving microvascular perfusion following hypertensive injury.
.
.
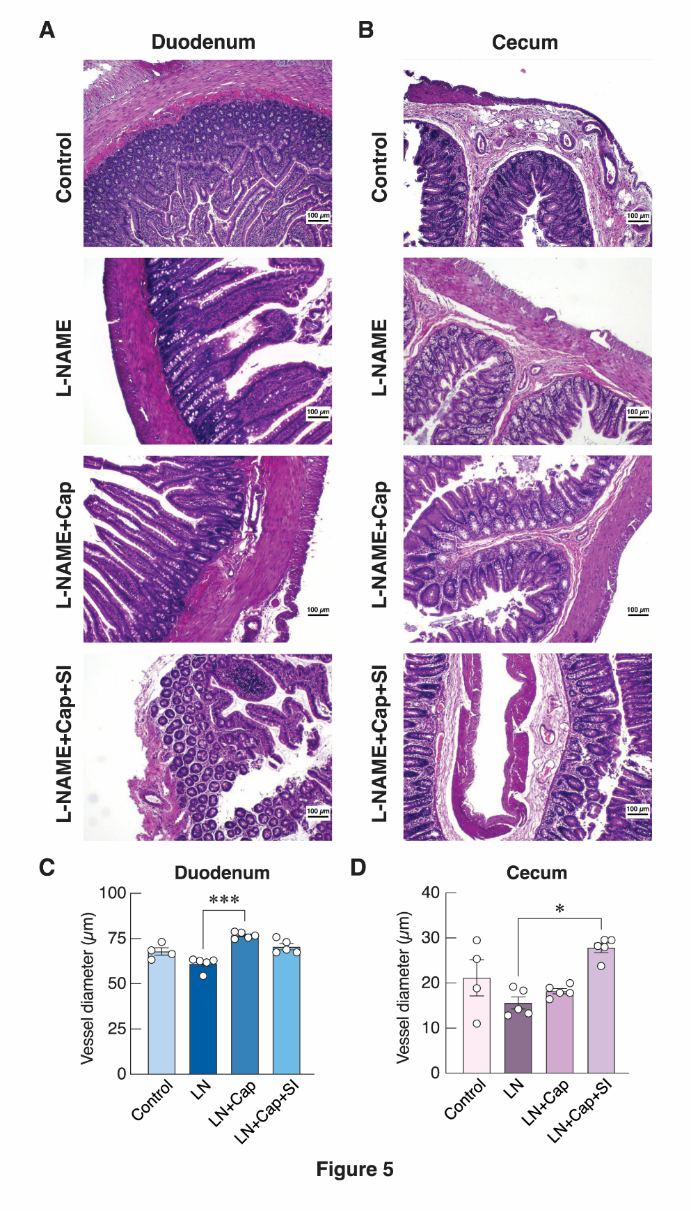
Figure 5 Histological and quantitative analysis of vessel diameter in the intestinal wall. (A) Representative histological images showing vessel diameter in the duodenal wall. (B) Representative histological images showing vessel diameter in the cecal wall. Images were obtained from the control, L-NAME, L-NAME + captopril, and L-NAME + captopril + Sacha inchi meal protein hydrolysate groups using a 100× microscope objective. (C) Quantitative measurements of vessel diameter in the duodenal wall. (D) Quantitative measurements of vessel diameter in the cecal wall. LN: L-NAME, Cap: Captopril, SI: Sacha inchi protein hydrolysate. Data are presented as mean ± S.E.M. Statistical significance among the four experimental groups is indicated as follows: *p < 0.05, and ***p < 0.001.
The present study demonstrates that vascular responses to hypertension and treatment interventions were region specific, with the duodenum and cecum exhibiting distinct patterns of microvascular remodeling. As expected, L-NAME administration significantly increased duodenal vessel diameter, consistent with previous reports indicating that chronic nitric oxide synthase inhibition promotes endothelial dysfunction, elevated vascular tone, and maladaptive vascular remodeling. The dilation observed in the duodenum may therefore reflect compensatory structural changes secondary to sustained hypertensive stress. In contrast, the cecal microvasculature showed a different pattern. The combination of captopril and Sacha inchi protein hydrolysate produced a significantly greater vessel diameter compared with L-NAME alone, suggesting enhanced microvascular adaptation in this region. This response may be attributable to the vasoprotective effects of ACE inhibition together with the potential antioxidant and anti-inflammatory activities of Sacha inchi-derived peptides, which collectively support improved endothelial function [20,22]. The observed enlargement of cecal vessels may represent either early vascular restoration or a compensatory remodeling process aimed at improving perfusion under hypertensive conditions. Thus, the biological interpretation of vessel diameter enlargement differs by intestinal region and disease state. Whereas duodenal dilation under L-NAME conditions likely represents maladaptive remodeling, the cecal response observed with combination therapy may indicate partial restoration of endothelial function or beneficial structural adaptation. These region-specific differences highlight the complexity of intestinal vascular regulation and suggest that combined nutraceutical-pharmacological approaches may differentially modulate microvascular architecture along the gastrointestinal tract.
Anti-inflammatory effects of combination therapy
The representative images of the inflammatory cell infiltration in the duodenum and cecum were shown in Figures 6(A) and 7(A). The number of inflammatory cells was assessed in the duodenal and cecal tissues to evaluate the extent of inflammatory responses among experimental groups.
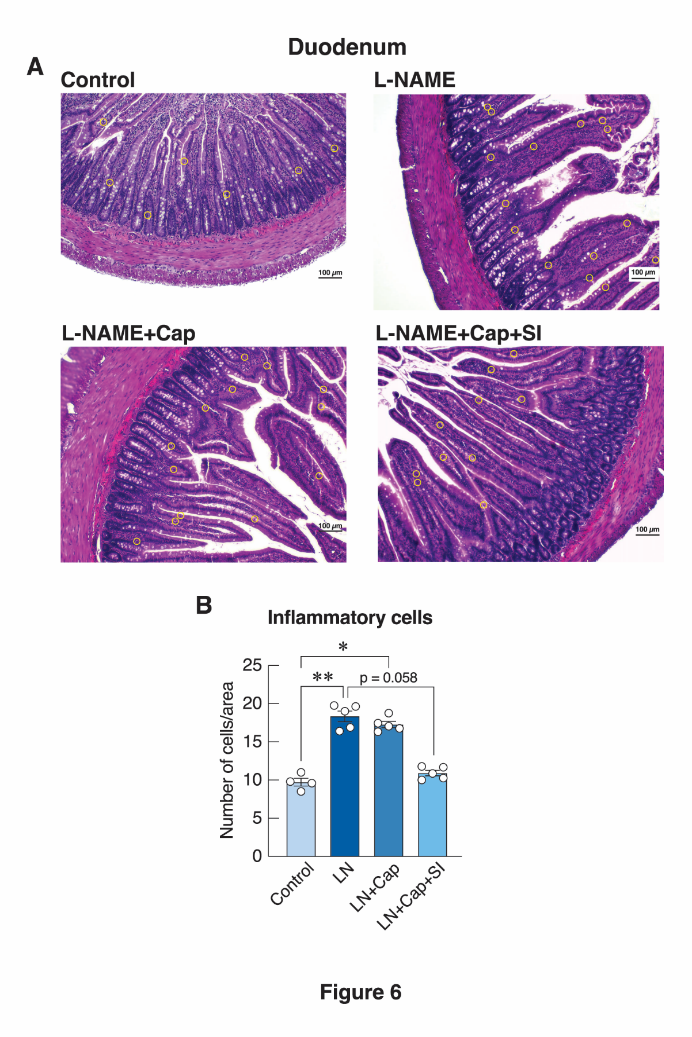
Figure 6 Histological and quantitative analysis of inflammatory cell infiltration in the duodenum. (A) Representative histological images of the duodenal wall showing inflammatory cells, indicated by yellow circles, in the control, L-NAME, L-NAME + captopril, and L-NAME + captopril + Sacha inchi protein hydrolysate groups. Images were captured at 100× magnification. (B) Quantitative analysis of inflammatory cell counts in the duodenum. LN: L-NAME, Cap: captopril, SI: Sacha inchi protein hydrolysate. Data are presented as mean ± S.E.M. Statistical significance among the four experimental groups is indicated as follows: *p < 0.05, and **p < 0.01.
Inflammatory cell analysis showed that both L-NAME and L-NAME + captopril groups had significantly elevated inflammatory cell numbers in the duodenum compared to control (p < 0.01 and p < 0.05, respectively; Figure 6(B)), indicating ongoing inflammation associated with hypertension and a partial reduction following captopril treatment. Similar patterns were observed in the cecum, where the L-NAME group exhibited significantly higher inflammatory cell counts than control (p < 0.01; Figure 7(B)). Although the combination therapy group demonstrated lower mean inflammatory cell counts compared with captopril monotherapy, this difference did not reach statistical significance (p = 0.058). This near-significant result suggests that the study may be underpowered to detect modest anti-inflammatory effects.
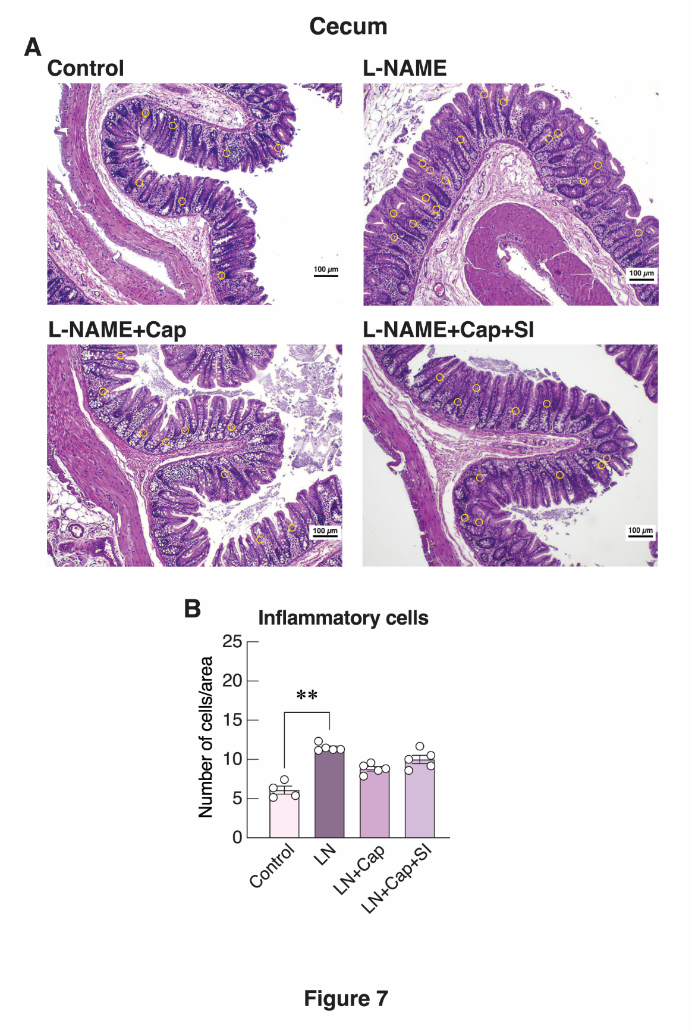
Figure 7 Histological and quantitative analysis of inflammatory cell infiltration in the cecum. (A) Representative histological images of the cecal wall showing inflammatory cells, indicated by yellow circles, in the control, L-NAME, L-NAME + captopril, and L-NAME + captopril + Sacha inchi protein hydrolysate groups. Images were captured at 100× magnification. (B) Quantitative analysis of inflammatory cell counts in the cecum. LN: L-NAME, Cap: Captopril, SI: Sacha inchi protein hydrolysate. Data are presented as mean ± S.E.M. Statistical significance among the four experimental groups is indicated as follows: **p < 0.01
The inflammatory profiles observed in the duodenum and cecum further underscore the detrimental effects of nitric oxide deficiency on intestinal homeostasis. L-NAME administration markedly increased inflammatory cell infiltration in both regions, consistent with previous findings that chronic NOS inhibition induces oxidative stress, compromises mucosal integrity, and promotes leukocyte recruitment [5,23]. The elevated inflammatory response in hypertensive rats highlights the sensitivity of the gastrointestinal mucosa to systemic vascular dysfunction. Captopril monotherapy partially attenuated inflammation in the duodenum, suggesting that ACE inhibition can mitigate some of the inflammatory consequences of hypertension, likely through reduced angiotensin II-mediated oxidative and pro-inflammatory signaling [24]. However, the persistence of significantly elevated inflammatory cell counts relative to controls indicates that captopril alone does not fully reverse the inflammatory burden. While a downward trend in inflammatory cell numbers was observed with the addition of Sacha inchi protein hydrolysate, this observation is best regarded as exploratory. Further studies with larger sample sizes and sufficient statistical power are required to determine whether combined pharmacological-nutraceutical intervention confers a meaningful anti-inflammatory advantage.
Lymphoid tissue response and immune modulation
Representative images of the lymphatic nodule expansion in the duodenum and cecum were shown in Figures 8(A) and 8(B). The lymphatic nodule area was assessed in the duodenal and cecal tissues to evaluate the extent of immune responses among experimental groups.
Lymphatic nodule analysis revealed significantly increased areas in the duodenum of L-NAME-treated rats compared to control (p < 0.01; Figure 8(C)), reflecting an upregulated immune response in hypertensive rats. In the cecum, captopril monotherapy significantly increased lymphatic nodule area compared to the control (p < 0.001; Figure 8(D)), suggesting enhanced immune surveillance potentially associated with captopril treatment.
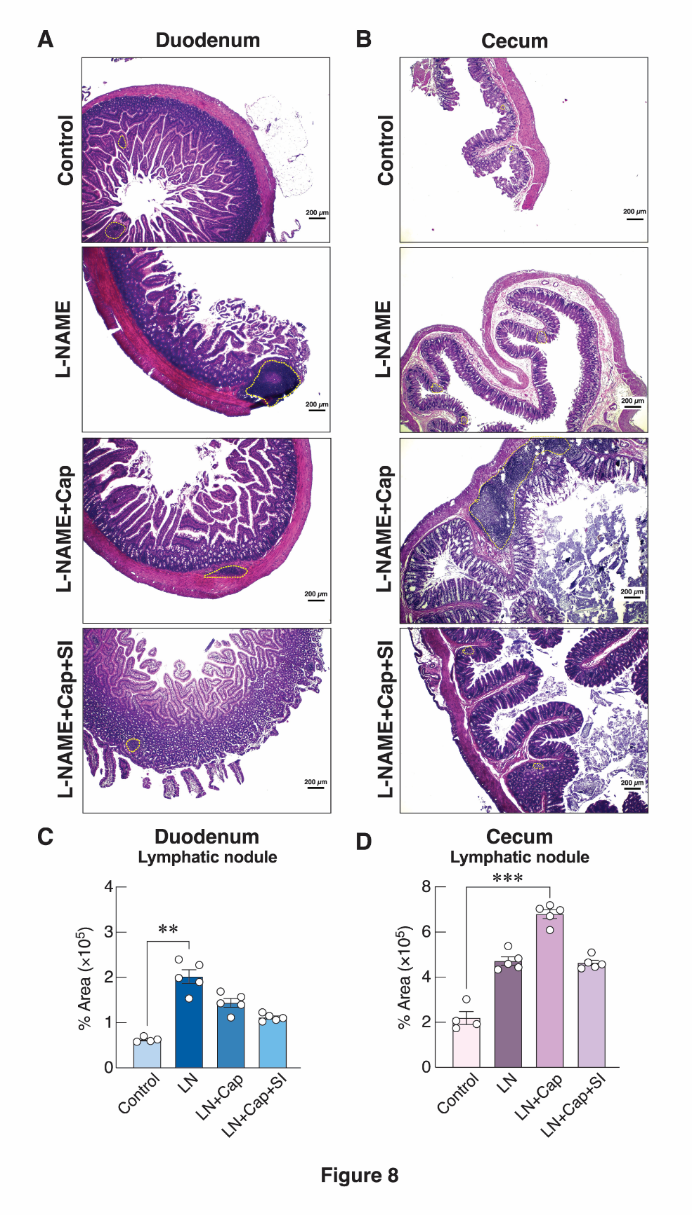
Figure 8 Histological and quantitative analysis of lymphatic nodule expansion in the intestinal wall. (A) Representative histological images showing lymphatic nodule expansion in the duodenal wall, indicated by yellow dashed outlines. (B) Representative histological images showing lymphatic nodule expansion in the cecal wall, indicated by yellow dashed outlines. Images were obtained from the control, L-NAME, L-NAME + captopril, and L-NAME + captopril + Sacha inchi protein hydrolysate groups using a 40× microscope objective. (C) Quantitative measurements of lymphatic nodule area in the duodenal wall. (D) Quantitative measurements of lymphatic nodule area in the cecal wall. LN: L-NAME, Cap: captopril, SI: Sacha inchi protein hydrolysate. Data are presented as mean ± S.E.M. Statistical significance among the four experimental groups is indicated as follows: **p < 0.01, and ***p < 0.001.
The expansion of lymphatic nodules in both the duodenum and cecum provides additional insight into the mucosal immune alterations induced by hypertension and its treatments. In the duodenum, L-NAME administration resulted in significantly enlarged lymphatic nodules, indicating heightened local immune activation. This response is consistent with the pro-inflammatory milieu associated with nitric oxide deficiency, which promotes epithelial stress, microbial imbalance, and enhanced antigenic stimulation of gut-associated lymphoid tissue (GALT) [25]. Such hypertrophy of lymphoid structures is frequently observed in models of chronic inflammation and has been linked to compensatory immune surveillance under physiological stress [26]. Interestingly, in the cecum, captopril monotherapy led to a significant increase in lymphatic nodule area compared with controls. This finding suggests a region-specific immunomodulatory effect of ACE inhibition. Captopril has been reported to influence immune cell trafficking, oxidative balance, and cytokine production, all of which may contribute to mild lymphoid hyperplasia [27]. The enhanced lymphatic nodule area may reflect either an adaptive strengthening of mucosal immunity or a response to ongoing but subclinical inflammation not fully resolved by pharmacological treatment. Taken together, these results highlight distinct patterns of GALT adaptation across intestinal regions in response to hypertension and therapeutic interventions. Whereas L-NAME primarily drives lymphoid activation through inflammatory pathways, captopril appears to modulate immune architecture in a more complex manner, possibly supporting immune readiness while concurrently reducing overt inflammatory cell infiltration. Further studies examining cytokine profiles and lymphocyte subpopulations would help clarify the functional implications of these structural changes.
Preserved goblet cell populations
Representative images of the goblet cells in the duodenum and cecum were shown in Figures 9(A) and 9(B). Goblet cell counts were evaluated in the duodenal and cecal mucosa to assess changes in mucus-secreting epithelial cells associated with hypertension and treatment effects.
Goblet cell analysis demonstrated notable alterations in mucosal epithelial composition following antihypertensive treatment. In the duodenum, captopril monotherapy significantly increased goblet cell numbers compared to L-NAME treatment (p < 0.001; Figure 9(C)), indicating a restorative effect of captopril on the mucosal barrier. Similar effects were observed in the cecum, where captopril treatment significantly increased goblet cells compared to both control and L-NAME groups (p < 0.001 and p < 0.05, respectively; Figure 9(D)).
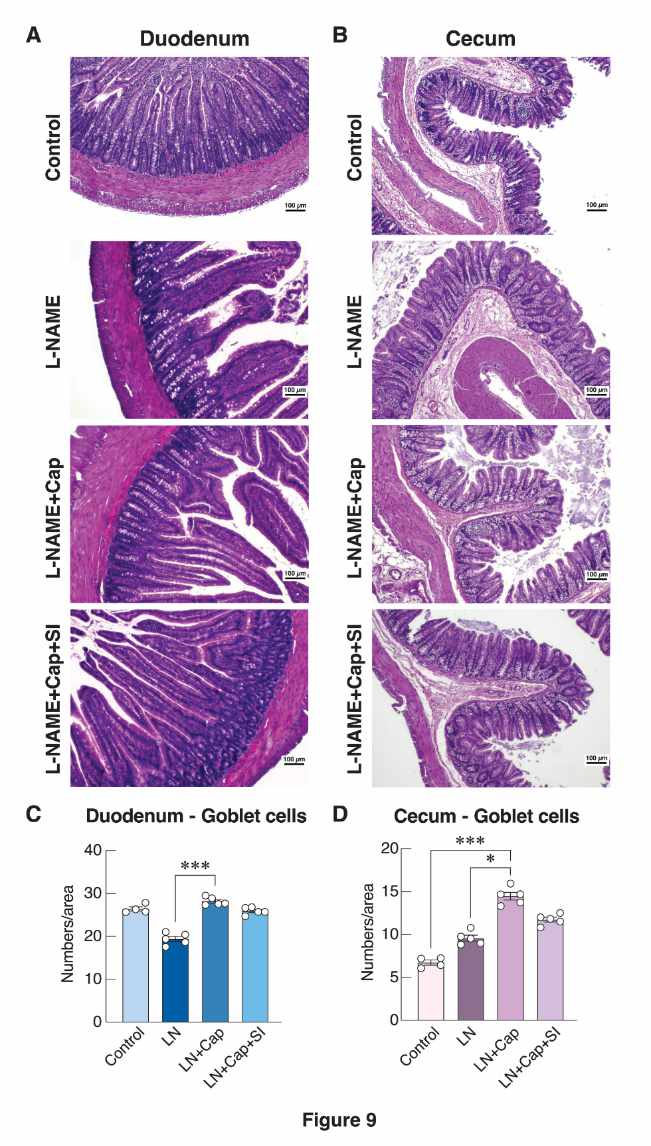
Figure 9 Histological and quantitative analysis of goblet cells in the intestinal wall. (A) Representative histological images showing goblet cells in the duodenal wall. (B) Representative histological images showing goblet cells in the cecal wall. Images were obtained from the control, L-NAME, L-NAME + captopril, and L-NAME + captopril + Sacha inchi protein hydrolysate groups using a 100× microscope objective. (C) Quantitative measurements of goblet cell number in the duodenal wall. (D) Quantitative measurements of goblet cell number in the cecal wall. LN: L-NAME, Cap: Captopril, SI: Sacha inchi protein hydrolysate. Data are presented as mean ± S.E.M. Statistical significance among the 4 experimental groups is indicated as follows: *p < 0.05, and ***p < 0.001.
Goblet cells are essential for maintaining the intestinal mucosal barrier through the production of mucins that form the protective mucus layer [28]. Changes in goblet cell density therefore provide meaningful insights into epithelial integrity under hypertensive conditions and therapeutic interventions. In this study, L-NAME-induced hypertension disrupted goblet cell populations, consistent with previous evidence that reduced nitric oxide availability promotes epithelial stress, oxidative damage, and impaired mucin secretion [29]. Captopril monotherapy significantly restored goblet cell numbers in both the duodenum and cecum, underscoring its capacity to modulate epithelial barrier-associated cell populations [17]. Notably, goblet cell density in the cecum exceeded that observed in healthy control animals. This supranormal increase should not be interpreted uncritically as purely beneficial. Rather, it may represent a compensatory or adaptive mucosal response aimed at reinforcing the mucus barrier in the context of persistent hypertensive or inflammatory stress. Alternatively, excessive goblet cell expansion may reflect altered epithelial differentiation or reactive mucin hypersecretion, phenomena that have been described in settings of chronic mucosal irritation [30,31]. Because functional assessments of mucus composition, epithelial proliferation, or differentiation markers were not performed, the present findings cannot distinguish between adaptive barrier strengthening and early pathological remodeling. Accordingly, the increased goblet cell density observed following captopril treatment is interpreted as an epithelial response indicative of altered mucosal homeostasis rather than definitive evidence of improved barrier function.
Enhanced collagen restoration in the duodenal and cecal wall with combination therapy
Representative images of the collagen deposition in the duodenum and cecum were shown in Figures 10(A) and 10(B). Collagen area was assessed in the mucosa, submucosa, and muscularis externa of both the duodenum and cecum to evaluate structural remodeling in response to hypertension and therapeutic intervention.
Collagen deposition analysis revealed that combination therapy significantly enhanced extracellular matrix restoration. In the duodenum, the combination group exhibited a significantly greater collagen area compared to L-NAME treatment (p < 0.05; Figure 10(C)), suggesting that the combined treatment may enhance extracellular matrix restoration or remodeling in hypertensive conditions. In the cecum, both combination therapy and control groups demonstrated significantly higher collagen areas than the L-NAME group (p < 0.01 and p < 0.05, respectively; Figure 10(D)), indicating successful restoration of structural integrity.
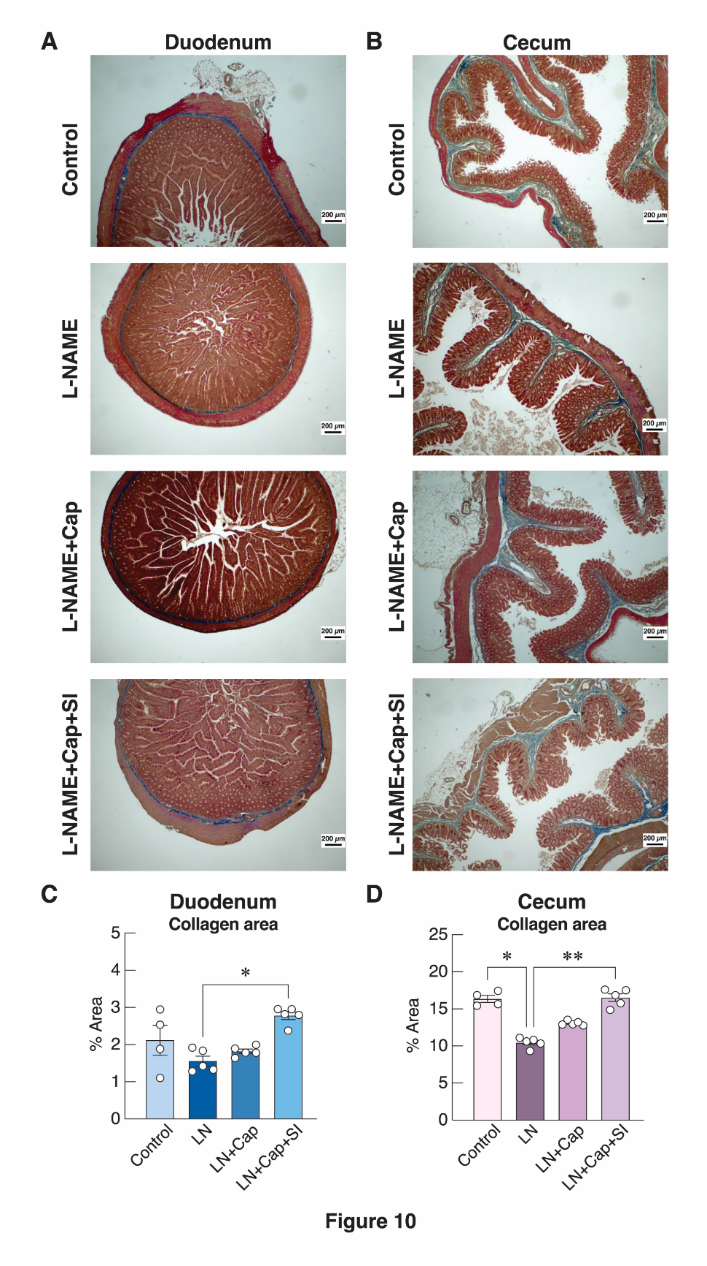
Figure 10 Histological and quantitative analysis of collagen deposition in the intestinal wall. (A) Representative histological images showing collagen deposition in the duodenal wall. (B) Representative histological images showing collagen deposition in the cecal wall. Images were obtained from the control, L-NAME, L-NAME + captopril, and L-NAME + captopril + Sacha inchi protein hydrolysate groups using a 40× microscope objective. Masson’s Trichrome staining was used to visualize collagen fibers. (C) Quantitative measurements of collagen area in the duodenal wall. (D) Quantitative measurements of collagen area in the cecal wall. LN: L-NAME, Cap: captopril, SI: Sacha inchi protein hydrolysate. Data are presented as mean ± S.E.M. Statistical significance among the four experimental groups is indicated as follows: *p < 0.05, and **p < 0.01.
Collagen deposition is a key determinant of intestinal structural integrity, contributing to tissue resilience, mechanical support, and proper mucosal function [32]. In this study, hypertension induced by L-NAME significantly reduced collagen content in both the duodenum and cecum, reflecting extracellular matrix (ECM) disruption commonly associated with hypertensive remodeling and oxidative stress. These alterations compromise intestinal architecture and may predispose the mucosa to injury or impaired barrier function [33]. Combination therapy with captopril and Sacha inchi protein hydrolysate significantly restored collagen deposition in the duodenum, suggesting enhanced ECM remodeling and mucosal reinforcement. In the cecum, both the combination therapy and control groups exhibited higher collagen areas than L-NAME alone, indicating effective structural restoration. These findings imply that Sacha inchi protein hydrolysate may potentiate captopril’s ability to promote ECM repair, possibly through modulation of collagen synthesis pathways, antioxidant activity, or inhibition of matrix-degrading enzymes [34]. Overall, the enhanced collagen deposition under combination therapy highlights its capacity to maintain or restore intestinal wall integrity under hypertensive stress, supporting the broader protective effects of nutraceutical-pharmacological co-therapy on gastrointestinal structure. Future studies could further explore molecular regulators of ECM remodeling, including collagen type expression, matrix metalloproteinases, and tissue inhibitors of metalloproteinases, to elucidate the underlying mechanisms.
In the summary, the intestinal structural alterations observed in this study can be interpreted within established mechanisms linking nitric oxide deficiency, renin–angiotensin system activation, and mucosal homeostasis. Chronic L-NAME exposure disrupts endothelial nitric oxide signaling, promoting angiotensin II-driven oxidative stress, microvascular dysfunction, and immune activation, which together contribute to mucosal thinning, collagen loss, and inflammatory infiltration. ACE inhibition with captopril mitigates these effects by suppressing angiotensin II signaling and improving vascular and epithelial stability, while bioactive peptides from Sacha inchi protein hydrolysate may further enhance antioxidant defenses and mucosal repair processes. Importantly, therapeutic responses differed between the duodenum and cecum, reflecting region-specific physiological contexts. The duodenum, characterized by high vascular density and rapid epithelial turnover, appears more sensitive to nitric oxide–dependent vascular and smooth muscle remodeling, whereas the cecum - rich in lymphoid tissue, microbial exposure, and mucus-dependent barrier function - exhibits pronounced adaptive responses in immune and epithelial compartments. These regional differences underscore that hypertensive injury and its modulation by combination therapy are not uniform along the gastrointestinal tract but are shaped by local vascular, immune, and epithelial demands. While the present study provides histological evidence that Sacha inchi protein hydrolysate enhances intestinal structural preservation during reduced-dose captopril treatment, several aspects warrant further investigation. Future studies incorporating larger sample sizes and both sexes will improve statistical robustness and generalizability. Inclusion of functional gastrointestinal outcomes, longitudinal assessments, and contemporaneous hemodynamic measurements would help clarify the relationship between intestinal remodeling and systemic blood pressure control. Mechanistic insight could be strengthened through molecular analyses targeting epithelial proliferation, stem cell activity, inflammatory signaling, oxidative stress pathways, and extracellular matrix regulation. Additionally, evaluation of systemic inflammatory markers, dose-response relationships, and multi-time-point analyses would refine interpretation of therapeutic dynamics. Collectively, these approaches will extend the translational relevance of the current findings and support the rational development of evidence-based nutraceutical–pharmacological combination strategies for hypertension-associated gastrointestinal alterations.
Conclusions
Sacha inchi protein hydrolysate, when combined with a reduced dose of captopril, was associated with preservation of intestinal structural integrity in L-NAME-induced hypertensive rats. The low-dose combination produced histological outcomes comparable to, and in selected parameters exceeding, those observed with full-dose captopril, particularly with respect to mucosal thickness, collagen deposition, and epithelial organization. These effects were observed at the tissue level and do not imply functional equivalence or established therapeutic substitution. Within the scope of this exploratory study, the findings provide proof-of-concept evidence that plant-derived bioactive proteins may complement conventional antihypertensive therapy by enhancing structural protection. Collectively, the results support further investigation of nutraceutical–pharmacological combinations to clarify functional relevance, dose-response relationships, and long-term outcomes before translational application.
Acknowledgements
This study was supported by University Income Fund, Naresuan University (Grant No. R2567C040). This work was also partially supported by the Reinventing University Program 2023-2025 from The Office of the Permanent Secretary of the Ministry of Higher Education, Science, Research and Innovation and Naresuan University, Thailand (Grant Nos. R2566A043, R2568A026, R2568A037), and the Global and Frontier Research University Fund, Naresuan University (Grant No. R2567C003). The authors acknowledge the Department of Anatomy, Faculty of Medical Science, Naresuan University, Thailand for providing laboratory facilities. We thank Asst. Prof. Dr. Ittipon Phoungpetchara and Asst. Prof. Dr. Pichaya Jumnongprakhon for scientific guidance, Mr. Phisid Saenganantakarn, and Ms. Sureeporn Nakung for technical assistance, and Professor Dr. Wai Chen for manuscript editing and English language review.
Declaration of generative AI in scientific writing
Artificial intelligence tools were used only to improve language clarity and readability; all study design, data analysis, and interpretation were performed solely by the authors.
CRediT author statement
Jarinthorn Teerapornpuntakit: Writing - original draft, review & editing; Visualization; Methodology; Investigation; Conceptualization. Tippaporn Bualeong: Supervision; Resources. Pakaporn Sa-nguanpong: Visualization; Methodology; Investigation. Worasit Tochampa: Resources. Khanitta Ruttarattanamongkol: Resources. Supawadee Auten: Methodology; Formal analysis. Pornpichaya Yottue: Methodology; Validation. Papichaya Bournoi: Methodology; Data curation. Pattarawadee Sawangwong: Methodology; Formal analysis. Hiroki Nakata: Writing - review & editing. Yutthapong Tongpob: Writing - review & editing. Charkriya Promsuban: Writing - original draft, review & editing; Validation; Project administration; Methodology; Investigation; Formal analysis; Conceptualization.
References
B Zhou, P Perel, GA Mensah and M Ezzati. Global epidemiology, health burden and effective interventions for elevated blood pressure and hypertension. Nature Reviews Cardiology 2021; 18(11), 785-802.
A Luqman, A Hassan, M Ullah, S Naseem, M Ullah, L Zhang, AU Din, K Ullah, W Ahmad and G Wang. Role of the intestinal microbiome and its therapeutic intervention in cardiovascular disorder. Frontiers in Immunology 2024; 15, 1321395.
P Sa-nguanpong, P Wetprasit, A Inchan, C Chaichana, W Kaewkong, N Charoenphon, K Adthapanyawanich, K Tantanarat, W Tochampa, K Ruttarattanamongkol and T Bualeong. Sacha inchi meal protein hydrolysate mitigates lipid accumulation and oxidative stress in HepG2 and 3 T3-L1 cells and synergistically enhances captopril's antihypertensive effects in L-NAME-induced hypertensive rats. Journal of Functional Foods 2025; 127, 106772.
M Choi, JR Hwang, JH Sung, N Byun, YS Seok, GJ Cho, SJ Choi, JS Kim, SY Oh and CR Roh. Hydroxychloroquine reduces hypertension and soluble fms-like kinase-1 in a Nω‑nitro‑L‑arginine methyl ester-induced preeclampsia rat model. Journal of Hypertension 2022; 40, 2459-2468.
P Sa-nguanpong, P Wetprasit, U Chatturong, K Chootip, N Kantip, W Tochampa, K Ruttarattanamongkol and T Bualeong. Protective effects of Sacha inchi meal protein hydrolysate against oxidative stress and endothelial dysfunction via MDA suppression and SOD activation in L-NAME-induced hypertensive rats. European Journal of Medicinal Chemistry Reports 2025; 15, 100297.
EY Rha, JW Kim, JH Kim and G Yoo. Angiotensin-converting enzyme inhibitor, captopril, improves scar healing in hypertensive rats. International Journal of Medical Sciences 2021; 18(4), 975-983.
J Zicha, Z Dobešová and J Kuneš. Antihypertensive mechanisms of chronic captopril or N-acetylcysteine treatment in L-NAME hypertensive rats. Hypertension Research 2006; 29(12), 1021-1027.
MN Takuathung, W Sakuludomkan, R Khatsri, N Dukaew, N Kraivisitkul, B Ahmadmusa, C Mahakkanukrauh, K Wangthaweesap, J Onin, S Srichai, N Buawangpong and N Koonrungsesomboon. Adverse effects of angiotensin-converting enzyme inhibitors in humans: A systematic review and meta-analysis of 378 randomized controlled trials. International Journal of Environmental Research and Public Health 2022; 19, 8373.
A Lemus-Conejo, A Villanueva-Lazo, ME Martin, F Millan and MC Millan-Linares. Sacha inchi (Plukenetia volubilis L.) protein hydrolysate as a new ingredient of functional foods. Foods 2024; 13, 2045.
K Wang, M He, Z Tan, X Tang, B Du and P Li. Arabinogalactan polysaccharides derived from sacha inchi shells alleviate angiotensin II-induced endothelial cell dysfunction. Carbohydrate Polymers 2025; 368, 124149.
N Kobayashi, D Takahashi, S Takano, S Kimura and K Hase. The roles of peyer's patches and microfold cells in the gut immune system: Relevance to autoimmune diseases. Frontiers in Immunology 2019; 10, 2345.
MJ Cano-Cebrian, D Dahlgren, F Kullenberg, K Peters, T Olander, M Sjoblom and H Lennernas. Chemotherapeutics combined with luminal irritants: Effects on small-intestinal mannitol permeability and villus length in rats. International Journal of Molecular Sciences 2022; 23, 1021.
SA Lawal, A Voisin, H Olof, M Bording-Jorgensen and H Armstrong. Diversity of the microbiota communities found in the various regions of the intestinal tract in healthy individuals and inflammatory bowel diseases. Frontiers in Immunology 2023; 14, 1242242.
MM Santisteban, Y Qi, J Zubcevic, S Kim, T Yang, V Shenoy, CT Cole-Jeffrey, GO Lobaton, DC Stewart, A Rubiano, CS Simmons, F Garcia-Pereira, RD Johnson, CJ Pepine and MK Raizada. Hypertension-linked pathophysiological alterations in the gut. Circulation Research 2017; 120(2), 312-323.
HJ Suh, HS Yang, KS Ra, DO Noh, KH Kwon, JH Hwang and KW Yu. Peyer's patch-mediated intestinal immune system modulating activity of pectic-type polysaccharide from peel of Citrus unshiu. Food Chemistry 2013; 138(2-3), 1079-1086.
B Li, X He, SS Lei, FC Zhou, NY Zhang, YH Chen, YZ Wang, J Su, JJ Yu, LZ Li, X Zheng, R Luo, D Kolodynska, S Xiong, GY Lv and SH Chen. Hypertensive rats treated chronically with Nω‑nitro‑L‑arginine methyl ester (L-NAME) induced disorder of hepatic fatty acid metabolism and intestinal pathophysiology. Frontiers in Pharmacology 2019; 10, 1677.
HB Li, T Yang, EM Richards, CJ Pepine and MK Raizada. Maternal treatment with captopril persistently alters gut-brain communication and attenuates hypertension of male offspring. Hypertension 2020; 75(5), 1315-1324.
T Bualeong, JM Wyss and S Roysommuti. Advances in Experimental Medicine and Biology 2019; 1155, 45-59.
S Suwanangul, RE Aluko, P Sangsawad, D Kreungngernd and K Ruttarattanamongkol. Antioxidant and enzyme inhibitory properties of sacha inchi (Plukenetia volubilis) protein hydrolysate and its peptide fractions. Journal of Food Biochemistry 2022; 46, e14464.
E Torres-Sánchez, I Lorca-Alonso, S Gonzalez-de la Fuente, B Hernandez-Ledesma and LF Gutierrez. Antioxidant peptides from Sacha Inchi meal: An in vitro, ex vivo, and in silico approach. Foods 2024; 13(23), 3924.
P Bryniarski, K Nazimek and J Marcinkiewicz. Immunomodulatory activity of the most commonly used antihypertensive drugs-angiotensin converting enzyme Inhibitors and angiotensin II receptor blockers. International Journal of Molecular Sciences 2022; 23(3), 1772.
JH Kim, H Kim, YH Kim, WS Chung, JK Suh and SJ Kim. Antioxidant effect of captopril and enalapril on reactive oxygen species-induced endothelial dysfunction in the rabbit abdominal aorta. The Korean Journal of Thoracic and Cardiovascular Surgery 2013; 46, 14-21.
M Majzunova, M Kvandova, A Berenyiova, P Balis, I Dovinova and S Cacanyiova. Chronic NOS inhibition affects oxidative state and antioxidant response differently in the kidneys of young normotensive and hypertensive rats. Oxidative Medicine and Cellular Longevity 2019; 2019(1), 5349398.
Z Gu, L Fang and P Ma. The angiotensin-converting enzyme inhibitor, captopril, suppressed hepatic stellate cell activation via NF-kappaB or wnt3α/β-catenin pathway. Bioengineered 2021; 12(1), 8370-8377.
JY Yoo, M Groer, SVO Dutra, A Sarkar and DI McSkimming. Gut microbiota and immune system interactions. Microorganisms 2020; 8(10), 1587.
M Balcerowska and P Kwasnik. The multifaceted impact of stress on immune function. Molecular Biology Reports 2025; 52(1), 1008.
S Brown, GDG Nores, A Sarker, C Ly, C Li, HJ Park, GE Hespe, J Gardenier, K Kuonqui, A Campbell, J Shin, RP Kataru, O Aras and BJ Mehrara. Topical captopril: A promising treatment for secondary lymphedema. Translational Research 2023; 257, 43-53.
S Yang and M Yu. Role of goblet cells in intestinal barrier and mucosal immunity. Journal of Inflammation Research 2021; 14, 3171-3183.
W Deng, M Zhu, I Lloyd, M Nedunuri, C Zhou, W Liu, Y Li, Q Li, X Wang, Q Zhang, TA Jhuma, J Li and T Yang. Beyond the microbiome: The gut's role in hypertension. Function 2025; 6(5), zqaf037.
I Brockhausen, D Falconer and S Sara. Relationships between bacteria and the mucus layer. Carbohydrate Research 2024; 546, 109309.
J Teerapornpuntakit, S Chatree, K Limpatchayopas, J Chamta, A Monteil and C Promsuban. Comparative histology of the swine colon raised under intensive management farming and backyard farming systems in Thailand. Trends in Sciences 2026; 23, 11188.
Z Wang, Y Wang, X Wang, G Zhao, H Zeng, H Xiao, L Han, J Ding, Y Chang and R Zuo. Vitamin E enhances immune function and the intestinal histological structure by regulating the nodal-mediated signaling pathway: A case study on the sea cucumber apostichopus japonicus. Biology 2025; 14(8), 1008.
M Vancamelbeke and S Vermeire. The intestinal barrier: A fundamental role in health and disease. Expert Review of Gastroenterology & Hepatology 2017; 11, 821-834.
CY Peng, AN Chen, ZZ Hu, MM Hu, HT Wang, HB Liu, J Cheng, ZY Xiong, Y Shi, Y Pan, XM Sha and ZC Tu. Comparative analysis of antioxidant activity and accelerated collagen expression of human skin fibroblasts with gelatin hydrolysates from different sources. Food Chemistry: X 2025; 29, 102850.